- Joined
- Oct 22, 2014
- Messages
- 62
- Reaction score
- 86
What are people making of the results presented at ASTRO this year? Do people want to follow the phase III evidence now or stick with retrospective MSKCC data? I don't treat prostate so curious.

I will still advise for 4-6 months of ADT in unfavorable intermediate risk PCA, but will sleep better at night if I cannot persuade the patients to follow my advice.What are people making of the results presented at ASTRO this year? Do people want to follow the phase III evidence now or stick with retrospective MSKCC data? I don't treat prostate so curious.
I think decreased mets and need for long term adt later is still worth it to someI will still advise for 4-6 months of ADT in unfavorable intermediate risk PCA, but will sleep better at night if I cannot persuade the patients to follow my advice.
SHared decision making. Describe the magnitude of the absolute benefit along with the risks and let men and their families decide. A rational human could decide either wayWhat are people making of the results presented at ASTRO this year? Do people want to follow the phase III evidence now or stick with retrospective MSKCC data? I don't treat prostate so curious.
What I see is 119 deaths in RT alone and 100 deaths in RT + ADT. Of those, 10 were cancer related in RT alone and 1 in RT + ADT. So, non-cancer is 109 vs 99 numerically favoring ADT.Are there excessive non-cancer deaths in the hormones arm? Something is suspicious here
From the presentation.What I see is 119 deaths in RT alone and 100 deaths in RT + ADT. Of those, 10 were cancer related in RT alone and 1 in RT + ADT. So, non-cancer is 109 vs 99 numerically favoring ADT.
I think this is only a one standard deviation difference, so it could just be a play of chance. Given such a low rate of cancer related deaths, there was not really any way that the study could be reasonably powered to show a 5 yr OS benefit. If it were a magic pill that erased cancer completely and we had double the sample size it still would not have been statistically significant in terms of OS. If the selection criteria had skewed towards younger patients unlikely to die of other causes it may have been possible to show OS benefit.What I see is 119 deaths in RT alone and 100 deaths in RT + ADT. Of those, 10 were cancer related in RT alone and 1 in RT + ADT. So, non-cancer is 109 vs 99 numerically favoring ADT.
Right. just answering the question re non-cancer related deaths. OS at 5 yrs is not worth talking about in this population. As far as I can tell, all the other outcomes seem to point to the longer term results looking the way they always have.I think this is only a one standard deviation difference, so it could just be a play of chance. Given such a low rate of cancer related deaths, there was not really any way that the study could be reasonably powered to show a 5 yr OS benefit. If it were a magic pill that erased cancer completely and we had double the sample size it still would not have been statistically significant in terms of OS. If the selection criteria had skewed towards younger patients unlikely to die of other causes it may have been possible to show OS benefit.
Indeed, but probably beyond 5 years.If the selection criteria had skewed towards younger patients unlikely to die of other causes it may have been possible to show OS benefit.
The adjuvant taxotere data suffered from the same problem, needed a better selected high risk population to show the benefit.
One major flaw in RTOG0815, apart from the primary endpoint in my humble opinion, is including all intermediate risk patients. They should have sticked to unfavorable intermediate risk.
UIR was not a thing in 2008 when the study was designedIndeed, but probably beyond 5 years.
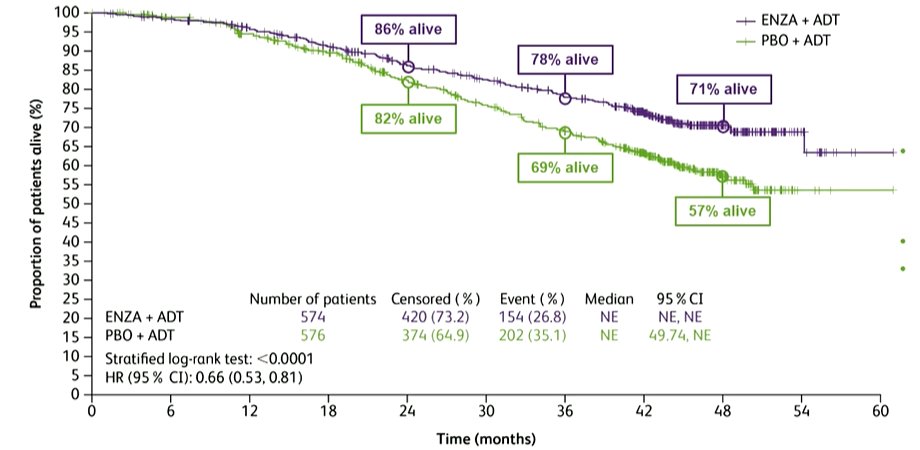
Median prognosis of metastatic prostate cancer nowadays is around 5 years. Here are the results of the ARCHES trial with ADT+Enzalutamide for mHSPC:
ESMO 2021: Final Overall Survival Analysis From ARCHES: A Phase 3, Randomized, Double-Blind, Placebo-Controlled Study of Enzalutamide + ADT in Men With mHSPC
ESMO 2021 Final analysis of the ARCHES trial of enzalutamide in men with mHSPC, enzalutamide + ADT significantly prolongs survival in men with mHSPC, abiraterone, apalutamide, or docetaxel.www.urotoday.com
Patients with localized prostate cancer who undergo RT without ADT, go on to develop biochemical progression and ultimately metastatic disease will live longer than that.
One major flaw in RTOG0815, apart from the primary endpoint in my humble opinion, is including all intermediate risk patients. They should have sticked to unfavorable intermediate risk.
One major flaw in RTOG0815, apart from the primary endpoint in my humble opinion, is including all intermediate risk patients. They should have sticked to unfavorable intermediate risk.
This is an important observation and I think it holds true for any intervention that is both fairly indiscriminate and effective. (There aren't as many of these as one would think, XRT in breast cancer, ADT in prostate and endocrine therapy in ER+ breast cancer come to mind). In the breast cancer setting, adjuvant XRT uniformly provides a local control benefit, but the absolute benefit is a function of age, cancer biology and receptor status.ADT provides pretty uniform risk reduction across the board, whether favorable intermediate or unfavorable intermediate, but your baseline risk is of course higher with unfavorable intermediate. If we had found for example that the recurrences with favorable intermediate just "happened" and ADT had no effect here then we could omit ADT, but that's not what the subgroup analysis showed
Almost none. No jokes, if it did, I wouldn't give anyone ADT. Go to Walmart. On a Saturday. You will see around 80% of my patient population.Question? How much does history of significant CAD (either history of MI or PCI) impact your recs for short course ADT in this setting?
Here it is. I'll be honest, I was a little surprised. I didn't think there was going to be much of any significant effect in the favorable group. However, I have always reasoned there could be and for the last couple years have discussed ADT for these guys in the context that it may help, I can't give them an exact number, and the absolute benefit will probably be small since most people will do well either way. This trial more or less confirmed my suspicions and really won't change my practice. I'll continue to offer but won't lose any sleep when people decline.The question to me is where we cross the threshold of excessively diminishing returns vs increased cost/toxicity. This is in turn different for each patient.
Is there any data out there suggesting that short-course ADT increases cardiac morbidity? I am only aware of data on long term ADT.Question? How much does history of significant CAD (either history of MI or PCI) impact your recs for short course ADT in this setting?
Hormonal Therapy Use for Prostate Cancer and Mortality in Men With Coronary Artery Disease–Induced Congestive Heart Failure or Myocardial Infarction (This was D'amico analysis from years ago)Is there any data out there suggesting that short-course ADT increases cardiac morbidity? I am only aware of data on long term ADT.
Perhaps RTOG 0815 will shed light into this?
I only read that Grade 3 late AEs were the same in both arms of RTOG0815 (16.2% in Arm 1 and 17.5% in Arm 2 (p=0.27)), but did they break it down to types of late AEs in the presentation?
 www.researchgate.net
www.researchgate.net