- Joined
- Feb 10, 2014
- Messages
- 202
- Reaction score
- 63
great system

Interestingly, this gave me a list extremely close to the list I am actually planning on applying to. It did tell me to through in a few more reaches than I am planning, but the bulk of my list was near identical.
Not sure if that is a testament to the accuracy of the model or the fact that I spend too much time on SDN.
")
Why do you consider shadowing not clinical experience? As far as I know, there are schools that do consider it clinical experience.
It is an excellent framework and probably the most thought out thing I've seen posted on SDN in a awhile. It could use some tweaks in my opinion though:
I think it gives too much stregnth to ECs. It would have someone with a 4.0 and a 33 MCAT with minimal shadowing and volunteering and not much else special about them applying to D.O. Schools only when really they have a great shot at most MD schools. The extremes of some of the ECs have issues too. Is being a minority really worth more than being an Olympic athlete or world class musician to adcoms? I'd assume the number of Olympic athletes and world class musicians entering medical school each year is <10. If the public recognizes your name for something positive I'd guess that's probably worth something like 40 points to some schools. I also don't think HYPS is worth double what UChicago or Duke or plenty of other schools are worth and "all other schools" is kind of a big range.
Why do you consider shadowing not clinical experience? As far as I know, there are schools that do consider it clinical experience.
There is a difference between following a doctor around and asking him questions and actually doing something yourself in a clinical setting.
There is a difference between following a doctor around and asking him questions and actually doing something yourself in a clinical setting.
Hi @WedgeDawg ,
Can you clarify what "adequate" shadowing means? Is it in terms of hours? Like 100+?
I'm closer to 80 hours, but should be up to 100 by the end of the summer. Additionally, I shadowed 3 physicians for 3 hours each, then did sustained shadowing with 2 other physicians. Not sure if this can change the "adequacy" of the shadowing experience or not.
Also, I'm not sure if my UG school is considered a 1 or a 2 - it's a Big Ten or "public ivy"
Finally, do you think it is possible to do something similar for MDPhD programs? I think other attempts have been made to collect this data but no attempt has been made to make it helpful to the application process like this.
THANK YOU! You smartypants, you.
Some people have a hook that sticks out, maybe their PS or one of their letters. At a certain point, you essentially get to flip a coin to see if you get an interview or not. The undergrad game is similar... only a few people get into all the Ivies every year, but many of them get into a top school.
They might have just liked someone with a similar app to yours over you. It happens. I applied to 45 schools and got 7-8 interviews. I was expecting to get interviews at about a quarter of places I applied to and I got a couple less. The timing of some of those interviews really surprised me as well since it felt like I was on the cusp for a lot of schools and many passed me over till the very last minute, including the school where I will likely be matriculating.
45??!! Oh my. How did you handle all those secondaries?? Props to you!ategory 6 (LOW YIELD): BU, Brown, Georgetown, Temple, Jefferson, GWU, Drexel, Penn State, Tufts, Tulane
Can someone explain why schools like BU, Brown, and Georgetown are in Category 6?
Those schools are the definition of category 6 (low yield).
The reason is that they are schools that are in great locations and are not exactly "elite" which means that everyone wants to go to them, the applicants who are mostly applying to top tier schools assume they are "safe", and applicants who aren't especially competitive think they are reasonable reaches. The end result is those schools getting inundated with applications, effectively decreasing the probability of getting in down near 1%.
As someone who is proud and excited to be starting Penn State next month, I have doubts as to whether I would consider Hershey a "great location"
4.0/33 with no shadowing, volunteering, or excellent ECs will definitely not get into "most MD schools".
They'll get a crap ton of secondaries, and probably a lot of interviews, and then they will put the interviewer to sleep...
I think it's in the eye of the beholder. I came from an urban undergrad and hated it- Hershey is awesome.As someone who is proud and excited to be starting Penn State next month, I have doubts as to whether I would consider Hershey a "great location"
Are you sure these are accurate ?Hello everyone! I have updated the OP with the newest old MCAT to new MCAT score conversions! The excel document (version 1.2) has also been updated to reflect this. Thank you all for your input and comments.
If anyone is curious, here are the conversions for each old MCAT score:
40+ = 523-528
39 = 522
38 = 521
37 = 519-520
36 = 518
35 = 516-517
34 = 515
33 = 514
32 = 512-513
31 = 510-511
30 = 509
29 = 507-508
28 = 505-506
27 = 503-504
26 = 501-502
Score conversions based on percentiles. I used the old score percentile as the minimum for the new score percentile so if
32 = 90th percentile
510 = 89th percentile
511 = 90th percentile
512 = 91st percentile,
then 32 = 511-512 (these numbers are made up)
You would have had a 521 and I would have had a 518.
It's not minimum, it's upper bound.Hello everyone! I have updated the OP with the newest old MCAT to new MCAT score conversions! The excel document (version 1.2) has also been updated to reflect this. Thank you all for your input and comments.
If anyone is curious, here are the conversions for each old MCAT score:
40+ = 523-528
39 = 522
38 = 521
37 = 519-520
36 = 518
35 = 516-517
34 = 515
33 = 514
32 = 512-513
31 = 510-511
30 = 509
29 = 507-508
28 = 505-506
27 = 503-504
26 = 501-502
Score conversions based on percentiles. I used the old score percentile as the minimum for the new score percentile so if
32 = 90th percentile
510 = 89th percentile
511 = 90th percentile
512 = 91st percentile,
then 32 = 511-512 (these numbers are made up)
You would have had a 521 and I would have had a 518.
@WedgeDawg You might want to consider adding state of residence as a factor (i.e. Ca is a negative, while Fl/Tx are a plus.) This is a huge factor in admissions. Just a suggestion...
I'll just add that their are many (well, like 8-9) states that are considered "lucky". In other words, your low stats won't keep you out of the home state med school. One of the best examples would be university of Mississippi, where the 10th percentile GPA is something like 3.2 and nearly half of her applicants get in! So yes, OOS odds do not change significantly from state to state (excluding tx). But, the odds of getting into a school do. The caveat is that you must be a resident to these states for some years before applying, obviously. I'd wager that they aren't stupid either, and that moving 12 months before application time is going to raise some eyebrows.Good suggestion! I thought about potentially doing something like this, but there aren't too many states where this would be a major factor (Texas being the biggest positive and NY/CA being the biggest negatives), so it would be hard to ascribe a point value to them. It also wouldn't really change your applicant level, just how hard your IS schools are to get into. An 'A' applicant from CA is still an 'A' applicant, regardless of how selective their IS schools are.
I'll just add that their are many (well, like 8-9) states that are considered "lucky". In other words, your low stats won't keep you out of the home state med school. One of the best examples would be university of Mississippi, where the 10th percentile GPA is something like 3.2 and nearly half of her applicants get in! So yes, OOS odds do not change significantly from state to state (excluding tx). But, the odds of getting into a school do. The caveat is that you must be a resident to these states for some years before applying, obviously. I'd wager they aren't stupid either, moving 12 months before application time isn't going to fool anyone.
Very true, as your system seems to be mainly designed for constructing an OOS list anyway.A very fair point, but it still wouldn't necessarily change the distribution of schools that you should apply to with your stats, other than perhaps making it so that you apply to fewer schools overall.
Are you going to add notes on particular schools?
For example Tufts really likes Tufts undergrads so for them, that is not a low yield school
What about SES status? for instance myself, I scored a 525 (100th)percentile mcat with a 3.99gpa. But I lived at 50% of the US poverty line, so I had to work full time, and take full time classes simultaneously. I'm applying this cycle, but I'm hoping schools may take my low SES combined with high stats with an extra grain of salt. You have URM on here, but not SES disadvantaged status is my point; they don't always correlate together. I think/I'm hoping, schools take low SES as a serious consideration.
btw @Goro, do you know whether low SES is actually even looked at or not?
I'll just add that their are many (well, like 8-9) states that are considered "lucky". In other words, your low stats won't keep you out of the home state med school. One of the best examples would be university of Mississippi, where the 10th percentile GPA is something like 3.2 and nearly half of her applicants get in! So yes, OOS odds do not change significantly from state to state (excluding tx). But, the odds of getting into a school do. The caveat is that you must be a resident to these states for some years before applying, obviously. I'd wager that they aren't stupid either, and that moving 12 months before application time is going to raise some eyebrows.
Edit: Just thought I would throw in this quote from UMC's website for anyone that gets any funny ideas lol
"Strong preference is given to applicants who are legal residents of Mississippi; in recent years, nonresidents have not been admitted. This medical school is committed to training health care providers for Mississippi. Moving to this state alone does not signify a commitment to practice in Mississippi. Applicants who recently move to Mississippi will be evaluated by the medical school admissions committee for their motivation to move and possible ties to this state."
Is averaging your sGPA and cGPA actually how Adcoms view your gpa?
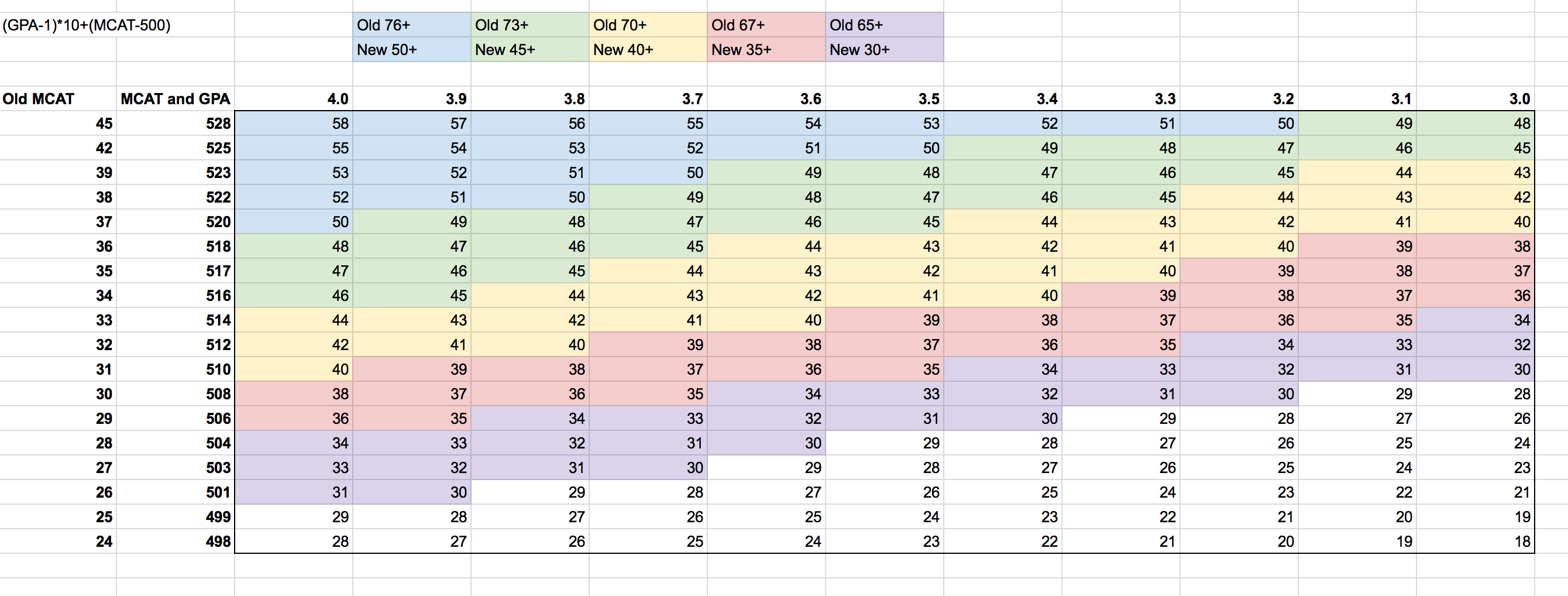
Alright guys, I have a proposed conversion for you all. The formula is:
(GPA-1)*10 + (MCAT-500) = Score
The max score (4.0/528) comes out to 58. I've gone through and made correlates between the old LizzyM score and the new one (which can be seen in the chart below). Examples:
Old 76 (i.e. 3.8/38 or 3.9/37) is new 50. This is generally the number to shoot for for top schools.
Old 73 (i.e. 3.8/35 or 3.9/34) is new 45. This is generally a good number for mid tiers while possibly being competitive for some top tiers.
Old 70 (i.e. 3.7/33 or 3.9/31) is new 40. This is generally where a "competitive" applicant for med school falls around.
Old 67 (i.e. 3.6/31 or 3.7/30) is new 35. This is around the accepted applicant median.
Old 65 (i.e. 3.6/29 or 3.7/28) is new 30. This is highly competitive for DOs and marginal for MD.
I didn't continue my color coordination after this, but you get the idea.
This score not only is easy to calculate, but provides convenient benchmarks for comparing scores to old LizzyM scores (down by 5's from 50 for new, down by 3's from 76 for old). It does break down at the MCAT extremes, but so did the old score (45/3.1 still gave you 76, for example).
Here are some spot checks:
3.7/32 is 69 old, which should be around 39ish new. Formula gives, for 3.7/512, 39, spot on!
3.4/38 is 72 old, which should be around 43-44 new. Formula gives, for 3.4/522, 46, so it's a little high, but it's also an extreme MCAT place.
3.9/32 is 71 old, which should be around 41-42 new. Formula gives, for 3.9/512, 41, right on!
3.3/36 is 69 old, which should be about 38-39 new. Formula gives, for 3.3/518, 41, so again, a little high.
This seems to work best the more "matched" the GPA and MCAT are, and gives slight favor to higher MCAT scores at the opposing extremes, but overall should be a decent estimate.
Obviously you can make it more accurate (by doing exact percentile conversions), but that would inevitably take away the simplicity of the calculation, which is the whole point. Also, because the new MCAT has multiple scores per old MCAT score, you're going to be hard pressed to find an algorithm that perfectly fits everything.
As we move away from old MCAT scores entirely, the conversion factor equality becomes far less important, and the balance between MCAT and GPA becomes the most important thing (here GPA is weighted out of 30 while MCAT is weighted out of 28, and the overall score can go as low as -32 if you have a 468 MCAT and 0.00 GPA). One MCAT point is still equivalent to 0.1 GPA points, just like the old scale.
See what you guys think!
Not sure how much this helps, but I was not recommended to apply to any of the low yield schools via this spreadsheet, but 2/4 of my II so far are from Gtown + BU..two low yield schools.
Other than that though, I think my distribution of schools is relatively similar of what is given.
Well these systems are good for informing your application choices, not dictating them. When it says "do not apply", it's not saying that you won't get interviews. I believe it just means that you will most likely not have to apply to them because you're projected get enough IIs from higher-yield schools (which you might very well find to be true later in the cycle).
Lol, would you apply to BU, Tufts, and/or G-town with those credentials?Meh you could post on SDN with a 4.0, 43, and a nobel prize and everyone would yell at you for applying to Georgetown/Tufts/BU.
Bumping this with the @WedgeDawg 2015 MCAT correction for the LizzyM score!.
Are we calling it the @WedgeDawg score? Speak now or forever hold your peace.
;-)