- Joined
- Aug 25, 2018
- Messages
- 538
- Reaction score
- 1,235
- Points
- 2,351
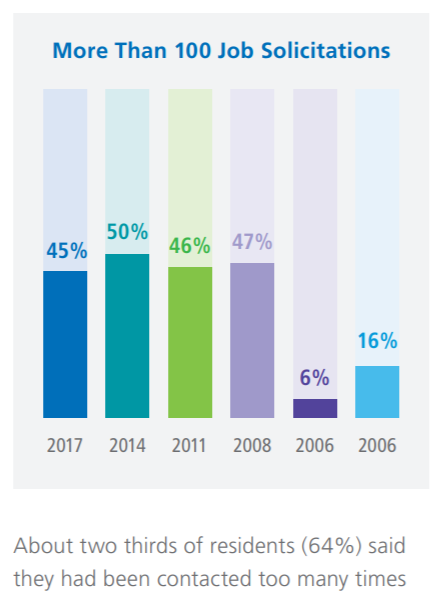
They definitely mixed this data up. This graph actually represents 100 job solicitations FROM the residents... not the other way around.

They definitely mixed this data up. This graph actually represents 100 job solicitations FROM the residents... not the other way around.
I personally know one of the former residents on that page and they also did a post residency fellowship but its not listed (site just states the current employer), lol. So that makes at least 4 of 12.Looking at their page, out of the past five years' worth of graduates, 3 went into fellowship: Our trainees - For Professionals | Northwell Health
There is one who was a research fellow but unsure if they continued on a research-based track or in straight clinical practice.
The calling started with the notion that a truly worthy radonc should be location agnostic, willing to live thousands of miles from family and friends.This is what "they" are counting on.
In American culture, it's relatively taboo to talk about salary. Doubly so with medical culture, with the added wrinkle that people often refer to it as a "calling" and whenever physicians indicate that they're human beings with wants and needs (like geography preferences), it can get quickly twisted into you "not doing what's best/right for your patients".
Throw into the mix: to successfully survive the gauntlet of education and training it requires to independently practice medicine in America, it requires years of making sure you're conforming to the system and only answering "how high" to the question of "jump", lest you not get a much needed "Honors" in a clerkship, a rec letter for residency, or a phone call on your behalf for a job.
This is how the system has evolved to where it is, RadOnc or otherwise. They'll continue to pay us just enough where we feel guilty voicing grievances. Compared to the prior generation of Radiation Oncologists, we get paid less (certainly in relative terms, and often in absolute terms), with less autonomy, and more paperwork. However, we still get paid significantly more than the average American household income, and so we feel bad about asking for more.
Isn't there the metaphor about frogs placed in a pot of warm water? It's like that.
I honestly hate the standing chair position model. Chair club serves nobody but chairs. I've commented on this before. Solution is rotating chairmanship for mid to late career physicians as an administrative duty with 3 year terms. This is how they do it in many non-medical departments. This takes away so much from the cult of personality bs and the conflating of being in an administratively powerful position and actually being a thoughtful or good doctor. This would actually help even relatively august academic places with retention of mid-career docs (not a problem in radonc for obvious reasons).Chair went on to ask if I'd be interested in a job in a city which met none of my criteria, working for another (overpaid) chair.
Sounds like you won. That chair conversation sounded awful. My chair didn't do jack for me or talk to me either. Would probably prefer that over them whoring me out to another chair as cheap attending labor, Hallahan styleWow. Your chair spoke to you? Like you were an actual human being? Interesting. Our department didn’t even discuss positions with us (in our out of our department). No phone calls were made.
I’m just tired of the same old fight.
The young generation tells us on paper that the landscape is good. Potters’ says things are fine and only a sock puppet and me respond. Nobody publicly will admit that they are working harder for less, that they have less autonomy, that admin is making their lives more difficult, that the day to day practice is not the same, that it’s fine.
I 100% agree, but if no one says this publicly, then the assumption is that we are anonymous and lying. People call me all sorts of things and blame all sorts of things on me. If nobody else says anything or backs me up, then I look like a liar. So, what's the point?Simul, it is a fight. I also interviewed recently as an experienced grad and made a lateral move (which seems to have been a step backwards). I can say confidently that there is much less opportunity now than there was a few years ago. Chairs and program directors are very upset, understandably, about declining applicant quality and are looking for someone to blame. The problem is that they specifically blame this website for spreading what they view as lies about there being no jobs and scaring applicants away. There's a disconnect here. They are believing something that isn't true, that people like us who have looked for work recently are lying and saying there are none. There are places that need rad oncs, definitely. Virtually all of us will be able to put food on the table with a 6 figure income. What we are saying is that the landscape has changed dramatically and that the opportunities that were there before aren't there anymore. Many areas of the country are essentially off limits. For instance, for myself, I can confidently say that there are no jobs for me in Florida. I have tried and tried. I will never get work there because of the names on my C.V. So are there really no jobs? Technically no, I can find work in Wisconsin. But not in Florida. And if by some miracle, I did ever get a call back from a Florida practice, it would be non-negotiable. The middleman between you and payors takes a bigger cut now because he can. This is what is scaring med students away. Not the lie that they will be unemployed and have to retrain in something else. There are plenty of other fields they can go into and make comparable amounts of money and find a job in Florida if they want it.
Ain’t no fun if the homies can’t have none.… whoring me out to another chair as cheap attending labor, Hallahan style
Beginning of PGY5 year, my chair offered me a position. I explained that I wanted to move closer to my (and partner's) family.Wow. Your chair spoke to you? Like you were an actual human being? Interesting. Our department didn’t even discuss positions with us (in our out of our department). No phone calls were made.
You're a brave man. You surely know that you have closed doors by putting your name out there. I hope I can get to that point one day. Unfortunately, I, like so many, can't afford to close doors in this market right now. I avoid lying, but I have learned when it's crucial to keep my mouth shut and when I can get away with presenting a different opinion. I have personally made the mistake before of calling out my superiors on obvious lies. While I was right and able to prove it, ultimately nothing I said or did hurt them, it only hurt me. They knew it was a lie, everyone knew it was a lie. So what did I accomplish by pointing out what everyone already knew? Luckily they just ignored me, but in retrospect, as a resident this was stupid -- I had far more to lose than to gain and I burned bridges over something trivial in the long run. So yeah, you are definitely hurting yourself and doing it knowingly, but the difference is I do think you are helping others in the long run. What you're doing is not stupid because you know and accept the risks up front and you're not doing it just for yourself. So that's admirable and worth something. Keep saying what you think -- it's important.I 100% agree, but if no one says this publicly, then the assumption is that we are anonymous and lying. People call me all sorts of things and blame all sorts of things on me. If nobody else says anything or backs me up, then I look like a liar. So, what's the point?
While many university hospitals are recovering 5x cms prices and chair salaries have exploded, you should be ashamed to expect median or historical radonc pay! And a job near family and friends? wtf you ungrateful bastard.When I was a brand new PGY5 just a few years ago, my very famous chair invited me to their office to discuss my job interests. I explained what I was looking for: community based practice, either freestanding or hospital based, open to satellites or hospital employment, and with an airport that had direct flights to the town where I trained (big city with >2M population). We reviewed my CV and cover letter, after which limited feedback was provided.
When asked about salary expectations, I said I hoped to make the ARRO average to start, and get up to median RO salaries as posted on MGMA etc within 5ish years.
Chair: (paraphrasing) "You're expecting too much. I think the days of radiation oncologists making that kind of money are over."
Chair went on to ask if I'd be interested in a job in a city which met none of my criteria, working for another (overpaid) chair. That was the extent of their involvement in my job search. No phone calls were made, no emails sent. Pretty cool. Luckily, I found a spot on my own that is working out well but definitely don't feel like I have any flexibility to move given these conditions.
I have always said that the next recession would prompt the "bad times" due to delayed retirements and practices belt tightening.I truly believe that an inflection point is coming and hard data re: bad times will be here soon. 'Til then we are climate modeling and forecasting really bad problems. And comparing to the past when things were awesome... things are easily much less awesome now, but they are not conflagrational. APM cancellation provided a respite.
More rad oncs are keeping upward pressure on the amount of money rad onc "costs" society; this cost would be falling were it not for rad onc over-supply (hypofractioning and decreasing RT utilization would mean less cost... these are hard facts and not predictions!). One ever increasing sign of rad onc over-supply, and a thorn in all of our sides, is more and more Evicore battling... and Medicare's APM fascination.
One thing is for certain: workforce studies, or papers on under- or over-supply, are COMPLETELY USELESS in rad onc. No one listens to data; everyone just will believe whatever one wants to believe to fit one's own narrative(s). There's a plethora of jobs in rad onc, and 2 solid job offers per graduating resident is 95% or more less job offers than residents in other specialties but 100% more job offers than one really needs!
Bad times can (will?) occur, but the gaslighting / "everything is fine" mentality will not change. Look at social media. As long as the charlatans continue to say everything is fine, get 200 likes and re-tweets, students won't know the difference. The applicant numbers have stabilized (forget about defining or talking about quality of candidates; irrelevant). No programs are contracting. We are probably a few years from further expansion. My guess is a few years from now, people that think like us will be further marginalized, the groupthink will persist and an ideal job will be 20 on beam, a low base, 10% quality incentives and this will be in not so great areas. And, the people that everyone will listen to will forget the past and say that this is how it always was and it's great.I have always said that the next recession would prompt the "bad times" due to delayed retirements and practices belt tightening.
People call me all sorts of things and blame all sorts of things on me.
He promptly got up and walked away without saying a word. Didn't speak to me the rest of the year, including a 3 month rotation with him.
🤮the groupthink will persist and an ideal job will be 20 on beam, $450k base, 10% quality incentives and this will be in not so great areas
If we didn't know what the landscape looked like 10-15 years ago, we probably wouldn't think this is too bad either.Bad times can (will?) occur, but the gaslighting / "everything is fine" mentality will not change. Look at social media. As long as the charlatans continue to say everything is fine, get 200 likes and re-tweets, students won't know the difference. The applicant numbers have stabilized (forget about defining or talking about quality of candidates; irrelevant). No programs are contracting. We are probably a few years from further expansion. My guess is a few years from now, people that think like us will be further marginalized, the groupthink will persist and an ideal job will be 20 on beam, $450k base, 10% quality incentives and this will be in not so great areas. And, the people that everyone will listen to will forget the past and say that this is how it always was and it's great.
Sorry, I think the gloomy weather has gotten to me.
You just described all employed jobs in the country's interior. It's not a bad life, but the problem is there is no upward mobility and the multiple levels of disassociation from what you do and how you get paid for your service causes people to just check out and become button clickers following guidelines and doing the bare minimum. It also allows administrators to slowly creep more work in for less pay over time.My guess is a few years from now, people that think like us will be further marginalized, the groupthink will persist and an ideal job will be 20 on beam, $450k base, 10% quality incentives and this will be in not so great areas.
So if a medstudent is happy earning a below than average physician salary in a location far from family and friends, then by all means, radonc calls. There is also the Worst case existential scenario where they end up unemployed, a risk which does not exist in the rest of medicine. Lots of interesting specialties to choose from.I think a big part of the angst on this board about jobs is where the current situation is, and where most people think the current situation ought to be if all was logical and fair in the world. I think the reality of the situation is that the salary and job security of the "golden years" will end up in the long run being the outlier situation. Some will say that it didn't have to be this way and that the bad actors in the field are responsible for ruining a great thing. They might be right, but no matter where the blame goes it doesn't change how things will look in the future. So comparing today's and tomorrow's jobs to yesteryear's is really a futile exercise - its never going back to that era. So even if today's jobs are comparatively objectively worse, it behooves people to judge them on their own terms independent of the past. Its almost like a kind of work inflation - your worth is less now than it was before and there's really nothing that can be done about it.
Nevertheless as it has been said in on this board many times, most of us actually like our jobs, so even if you are pessimistic about the future and feel like the pay is not fair compared to what we "should" get paid, I can understand why a med student would still want to do it - because at the end of the day the job itself is a pretty sweet gig (meaningful outpatient work with no nights or weekends will always be desirable).
Basically my job now. No way anything in the speciality changes for the better moving into the future on a macro level. Best case we can tread water for awhile and not lose ground. The math of shrinking footprint while pumping out more grads then docs retiring is inescapable as gravity. The people in a position to change this do not care. Save aggressively and develop other interest so you can FIRE out when you choose to.Bad times can (will?) occur, but the gaslighting / "everything is fine" mentality will not change. Look at social media. As long as the charlatans continue to say everything is fine, get 200 likes and re-tweets, students won't know the difference. The applicant numbers have stabilized (forget about defining or talking about quality of candidates; irrelevant). No programs are contracting. We are probably a few years from further expansion. My guess is a few years from now, people that think like us will be further marginalized, the groupthink will persist and an ideal job will be 20 on beam, $450k base, 10% quality incentives and this will be in not so great areas. And, the people that everyone will listen to will forget the past and say that this is how it always was and it's great.
Sorry, I think the gloomy weather has gotten to me.
Well.. it’s you and other people here that say this. And I believe you. This just gives credence to what I’ve been saying the last few days. Nobody says this publicly and non anonymously. So, basically it doesn’t exist - “angry internet people”. The surveys and the popular people say it’s fine. So, it’s fine. Until there are real faces saying it’s bad out there, it’s just rumors / “SDN” making stuff up. I don’t mean to say you are. Just perception.Basically my job now. No way anything in the speciality changes for the better moving into the future on a macro level. Best case we can tread water for awhile and not lose ground. The math of shrinking footprint while pumping out more grads then docs retiring is inescapable as gravity. The people in a position to change this do not care. Save aggressively and develop other interest so you can FIRE out when you choose to.
People say it in private all the time, med students come on here and have said as much when they are applying/rotating through the field.Well.. it’s you and other people here that say this. And I believe you. This just gives credence to what I’ve been saying the last few days. Nobody says this publicly and non anonymously. So, basically it doesn’t exist - “angry internet people”. The surveys and the popular people say it’s fine. So, it’s fine. Until there are real faces saying it’s bad out there, it’s just rumors / “SDN” making stuff up. I don’t mean to say you are. Just perception.
Doesn’t matter. Applicant numbers stabilized. Surveys say there are jobs.People say it in private all the time, med students come on here and have said as much when they are applying/rotating through the field.
Obviously it isn't just a bunch of angry anonymous internet malcontents that have tanked the match multiple years in a row now??
It is a different time now and any slot is a good slot to the right applicant.Doesn’t matter. Applicant numbers stabilized. Surveys say there are jobs.
That is so interesting that you think the match was tanked. How many spots weren’t filled after SOAP?
But, okay …
Plenty of anecdotal evidence to support this regarding many grads from the 70s and 90sI can’t prove this, but I am quite sure that most the American MDs in the match are not very intelligent/utter tools or both. Qualitatively I have heard this comes through via eloquence of candidates during interviews.
this is why no one takes the board seriously when people say they want to try to help med students make the right career choices etc. People come on the board to vent and convince others they are right and other people are wrong.I can’t prove this, but I am quite sure that most the American MDs in the match are not very intelligent/utter tools or both. Qualitatively I have heard this comes through via eloquence of candidates during interviews.
Yeah clearly no one has been taking this board seriously and the match has been totally normal since 2019 🙄this is why no one takes the board seriously when people say they want to try to help med students make the right career choices etc. People come on the board to vent and convince others they are right and other people are wrong.
You are deep in your career coming on a website called Student Doctor Network calling med students utter tools because you don't agree with their decisions, I think it probably says more about you than themYeah clearly no one has been taking this board seriously and the match has been totally normal since 2019 🙄
Says the guy who's been sticking his head in the sand the last few years wrt to the match and the specialty at large? You're the one who actually has to deal with this, being in academics and all 😂. At least you aren't talking about expansion or telling us contraction is a waste of time anymore though.... WhewYou are deep in your career coming on a website called Student Doctor Network calling med students utter tools because you don't agree with their decisions, I think it probably says more about you than them
My guess is a few years from now, people that think like us will be further marginalized, the groupthink will persist and an ideal job will be 20 on beam, $450k base, 10% quality incentives and this will be in not so great areas. And, the people that everyone will listen to will forget the past and say that this is how it always was and it's great.
You just described all employed jobs in the country's interior. It's not a bad life, but the problem is there is no upward mobility and the multiple levels of disassociation from what you do and how you get paid for your service causes people to just check out and become button clickers following guidelines and doing the bare minimum. It also allows administrators to slowly creep more work in for less pay over time.
I think these three posts basically summarize where we are, and where we're headed.I think a big part of the angst on this board about jobs is where the current situation is, and where most people think the current situation ought to be if all was logical and fair in the world. I think the reality of the situation is that the salary and job security of the "golden years" will end up in the long run being the outlier situation. Some will say that it didn't have to be this way and that the bad actors in the field are responsible for ruining a great thing. They might be right, but no matter where the blame goes it doesn't change how things will look in the future. So comparing today's and tomorrow's jobs to yesteryear's is really a futile exercise - its never going back to that era. So even if today's jobs are comparatively objectively worse, it behooves people to judge them on their own terms independent of the past. Its almost like a kind of work inflation - your worth is less now than it was before and there's really nothing that can be done about it.
And so? Spots are filled. Don’t what to tell ya. The problem is - there is no mechanism that doesn’t rely on people speaking openly / honestly to help change things. Potters goes out there with a complete clown comment, bro and it’s me and Ridge and then utter silence. How can change happen?
To be fair, the median physician salary is $206kmedian physician salary is $206kSo if a medstudent is happy earning a below than average physician salary in a location far from family and friends, then by all means, radonc calls. There is also the Worst case existential scenario where they end up unemployed, a risk which does not exist in the rest of medicine. Lots of interesting specialties to choose from.
In the original limb xrt sparing sarcoma trials, I thought there was no qol difference between amputees and limb preservation arm. Amputees were just so happy to be cancer free.
Ok I won't get too far down the rabbit hole here but you're linking the US News "median physician salary". So immediately we should ask "where does this number come from? It's not quickly apparent, but evidently it's from the Bureau of Labor Stats.To be fair, the median physician salary is $206k
$206k is NOT median physician salary.Ok I won't get too far down the rabbit hole here but you're linking the US News "median physician salary". So immediately we should ask "where does this number come from? It's not quickly apparent, but evidently it's from the Bureau of Labor Stats.
So now let's go to the BLS and look at their salary data.
Well clearly there's a wide range based on specialty:
View attachment 347057
Let's drill down here:
View attachment 347058
What could the [5] hyperlink bring us to, as it indicates the median income and higher?
View attachment 347059
So if a job hits at least $100 per hour, BLS throws their hands in the air? Ergo, for high paying jobs the median is around $208k?
I don't want to dig deeper, so if someone else feels like it, let us know. I don't know if US News is my go-to for doctor salary references though.
Fake news. No way median salary in 206k. Methodology..To be fair, the median physician salary is $206k
This statement is so spot on. It’s hard to see yourself as someone who used to describe yourself as ambitious but then the vanilla has sucked you dry for a couple of years and you’re not really sure what to do about it or what kind of pivot to make. It’s a really challenging situation.hose personalities are, on average, ambitious, and have expectations for their future. Even if the system has elasticity to keep new grad unemployment low, that "employment" is potentially a very vanilla prospect, with a tight ceiling and floor on salary, limited room for growth (or intentional shrinkage), significant dependence on a referral chain, and extremely limited geography.

 www.beckersasc.com
www.beckersasc.com
These numbers are closer, but if you drill down here too, they're from Doximity, and they're averages, which is very important.10 highest-paid physician specialties - Becker’s ASC
Neurosurgery boasts the highest compensation of any physician specialty, according to Doximity's "2021 Physician Compensation Report" released Dec. 16.
Most rad onc salary surveys I've ever seen are less than 100 respondents. I remember one year the MGMA data was based on less than 40 rad oncs.There are definitely some "whales" in the RadOnc salary surveys
I am not an economist thus I wouldn't know how to evaluate their methodology. I will, however, point out that this is what a number of surveys report, including government sourcesFake news. No way median salary in 206k. Methodology..
Are you really trying to double down on 206k being average physician salary? Move onI am not an economist thus I wouldn't know how to evaluate their methodology. I will, however, point out that this is what a number of surveys report, including government sources
Do you have a trusted source that points to a median physician salary that is vastly different?
Not doubling down per se... I would be comfortable moving on if someone had some stats to dispute it rather than simply dismissing it out of hand.Are you really trying to double down on 206k being average physician salary? Move on
In many locations with radonc availability (satellite in kentucky, or iowa), we would be the lowest paid specialist.Are you really trying to double down on 206k being average physician salary? Move on
this is nonsenseIn many locations with radonc availability (satellite in kentucky, or iowa), we would be the lowest paid specialist.
No academic is going to be concerned about grads who don't go into academics making ~400K with limited geographic options. The money remains good in radonc at present relative to many fields (I make much more than my PCP spouse, who works hard), although not what it once was. Academics typically view themselves as choosing to make less money by going into academics and don't perceive (although they are) that they are hurt by diminishing PP opportunities.So, everyone just needs to recalibrate their expectations in BOTH directions, and perhaps something will be invented in 2030 that recaptures the bottled lighting that IMRT was in 2000.