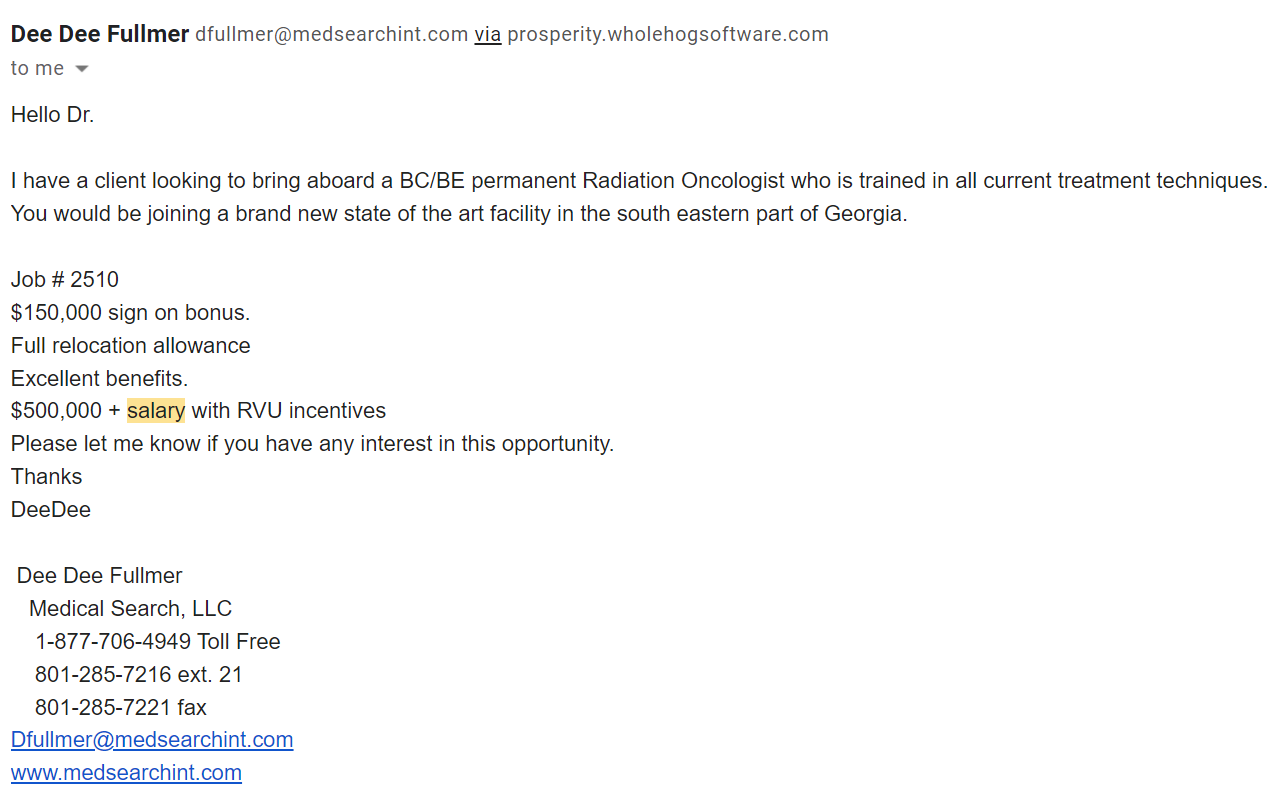
Perhaps average physician SALARY is $208k. But have you met his friend, Mr. BONUS? He's the really, really big guy standing next to SALARY.
If you actually believe that the average American physician grosses out 200k, I'd wonder if you are actually a physician.
I don't know what the average salary is across all specialties, but for primary care (outpatient IM, family med, peds) in a coastal, major urban area, $200K is probably about the highest that you're going to go without doing something extra - seeing a ton of patients, working six days a week or extended evening hours, nursing home rounds, doing both outpatient AND inpatient, etc. In a place like NYC or Boston, $200K is probably being a bit generous.
Midwestern major urban areas are probably a touch higher, but not by a huge amount. Midwestern mid-sized urban areas are higher, and rural areas (midwest, mountain states, southeast) are the highest of all, obviously.
Peds will be even less.
None of this should be a surprise, though. I feel like these numbers and trends are common knowledge on SDN by now.
Any time I see data (a website with someone’s salary) like this I think… what am I missing. I guess people go into medicine now with all its hurdles and hassles to make less than what they could more easily and quickly make in other fields. Wild stuff.
I feel like this incredibly naive or disingenous. Can you really not wrap your mind around why someone would go into medicine (yes, even with its hurdles and hassles) to make less than they could in other fields?
This is like the old trope of a roomful of old white guys debating why women would want to vote.
As someone who has been in primary care for over a decade, here are my reasons:
- I don't have the attention span to be a specialist. Call it attention span, mentality, mindset, whatever - I don't have it.
As residents, we would have to spend a month in the outpatient office of various specialties. There were 3 phases for me:
1) "Ohhh, this specialty is awesome! I should have done THIS instead!")
2) "Well, the shine has worn off, but it's still pretty cool."
3) "OMG, if we talk about BPH/gastritis/CHF/COPD/cataracts/bread-and-butter issue for that specialty one more time, I'm going to rip my f***ing ears off."
There were also some specialties where phase 1 never happened (Emergency medicine and outpatient ENT, I'm looking at you. Nothing against the specialties, just not for me.)
- Flexibility. As a rad onc, you're tied to either a large hospital that can afford the expensive machinery that you guys need, or a major corporation (21st Century, Cancer Treatment Centers of America) that can. As a BC family med physician, I can do so many things if I wanted to, and can work in literally almost any location in the world. I can do urgent care, hospitalist, community clinics, locums, part time, full time, off hours, and now telemedicine. If I have to pick up and move to Alabama tomorrow, I'll be able to find a job. If we had to move to Manhattan, I could find a job.
- I genuinely believe that healthcare should be for everyone - young, old, rich, poor, undocumented or not. I really don't care. But this healthcare system is hard to navigate for the average lay person and many specialists do not always take the time to explain things. I get a lot of satisfaction out of making complicated things clear and understandable.
- I genuinely believe that prevention the optimal strategy. Some of the cancers that you treat are unavoidable, but don't you guys ever feel a pang of sadness when you treat a patient with a cancer that could have been avoided? Like advanced cervical or colon cancer? Or HPV-mediated anal/rectal cancers? I know it sounds like the usual lip service that you write about on your personal statement to get into medical school, but preventing bad diseases honestly matters to me.
I don't need a lot of money. I don't have expensive tastes in cars, or jewelry, or vacations. Even "only" $200K is plenty.