You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
alines for ablations
Started by Gas you down

This coming from the other thread?
We did it for all of them in fellowship and that continues at my current gig. Most have a lot of hemodynamic swings as they do the ablation and it’s an intracardiac procedure. Slam dunk a-line indication - minimal risk in placement and a lot of benefit.
Some of our cardiologists prefer to place femoral a-lines that we hook into for monitoring, which is fine by me. Most also give us a line off their central access as well, if asked for difficult access. Easy!
We did it for all of them in fellowship and that continues at my current gig. Most have a lot of hemodynamic swings as they do the ablation and it’s an intracardiac procedure. Slam dunk a-line indication - minimal risk in placement and a lot of benefit.
Some of our cardiologists prefer to place femoral a-lines that we hook into for monitoring, which is fine by me. Most also give us a line off their central access as well, if asked for difficult access. Easy!
We always did routine alines for Afib ablations under general. not so much for aflutter/svt ablations. My current gig rarely does them at all in EP. what is your practice?
No a lines.
I would not consider a fib ablations as a hemodynamically unstable procedure.
Advertisement - Members don't see this ad
Nope. Not routine.
didn't know about another thread. only started doing EP a few years back when we built a lab. this was the recipe provided to us at the time. i assumed you had hemodynamic instability when they're trying to pinpoint their target.
D
deleted162650
A-line/GA for any procedure where they’re crossing the septum. MAC and RM only for procedures staying on the R-side only.
Where I am currently the majority of our ablations are done MAC and the a-lines are patient specific and more often than not we do not place any.
No a line for a fib ablations here unless very sick.
We routinely do, and I'm glad. Just 2 weeks ago we had an atrial burn through to emergent sternotomy. Very rare, but it definitely helped my partner who it happened to (Afib ablation).
A-lines generally for a-fib. Not for A flutter. Both usually get TEEs to interrogate the appendage.
Advertisement - Members don't see this ad
No A line, do tons of them. Maybe if the person has structural heart disease on top of the arrythmia or severely depressed EF. IMO patients rarely get that hypotensive during periods of pacing and mapping.
Certainly have had my fair share of iatrogenic effusions/tamponade in the Cath lab.
We had one a couple weeks ago.Certainly have had my fair share of iatrogenic effusions/tamponade in the Cath lab.
I put a-lines in all of the afib ablations I do.
Certainly have had my fair share of iatrogenic effusions/tamponade in the Cath lab.
i guess it depends on how good the proceduralists are at different places.
i like to see the pressure when they're giving Isuprel or adenosine
I put an Aline in every PVI as do all of my partners. We do 3-4 per day. It was done this way in residency and fellowship as well.
Definite BP swings with isoprel, periods of pacing, and the occasional effusion.
Definite BP swings with isoprel, periods of pacing, and the occasional effusion.
We do them 100% of the time. They are requested by the cardiologists.
Never done one for an Afib ablation.
Interesting to see such a difference in practice; that doesn't occur for too many procedures in anesthesia.
Interesting to see such a difference in practice; that doesn't occur for too many procedures in anesthesia.
Advertisement - Members don't see this ad
I don't worry about IV access as much, I just take the venous sheath in an emergency
Never done one for an Afib ablation.
Interesting to see such a difference in practice; that doesn't occur for too many procedures in anesthesia.
You ever done an afib ablation with a patient who has PA systolics in the 90-130 range? What would you worry about?
i guess it depends on how good the proceduralists are at different places.
and how many you do and how sick and old your patient population may be.
They are usually fine, until they are not. And at that time their hands are tucked.
I'm not saying every center needs an a-line for afib ablation, but there is no harm in doing one if that is your set up. Good upside with very little downside.
It's a 2 minute procedure and an afib ablation can take a while. Intracardiac procedure, poking around, burning, transeptal, sick patients...
It's a 2 minute procedure and an afib ablation can take a while. Intracardiac procedure, poking around, burning, transeptal, sick patients...
Last edited:
You ever done an afib ablation with a patient who has PA systolics in the 90-130 range? What would you worry about?
Hey, at least their RV is strong enough to generate those pressures!
No a line for a fib ablations here unless very sick.
Yeah. The case doesnt require it.
No, never done them on sick patients: they all seem to be middle age over weight with aceptable cardiac function.You ever done an afib ablation with a patient who has PA systolics in the 90-130 range? What would you worry about?
D
deleted697535
A line for 100% of ablations. We get about 2 tamponades a month
Advertisement - Members don't see this ad
No, never done them on sick patients: they all seem to be middle age over weight with aceptable cardiac function.
Most of my patients have multiple cardio-pulmonary comorbities.
This is what can happen:
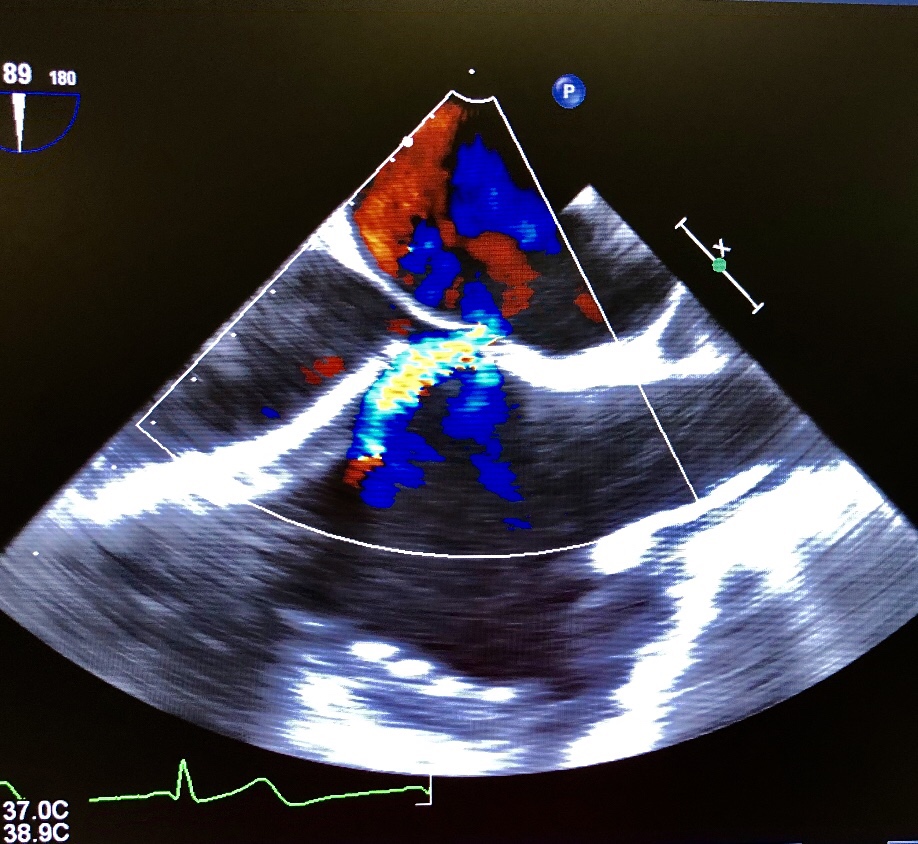
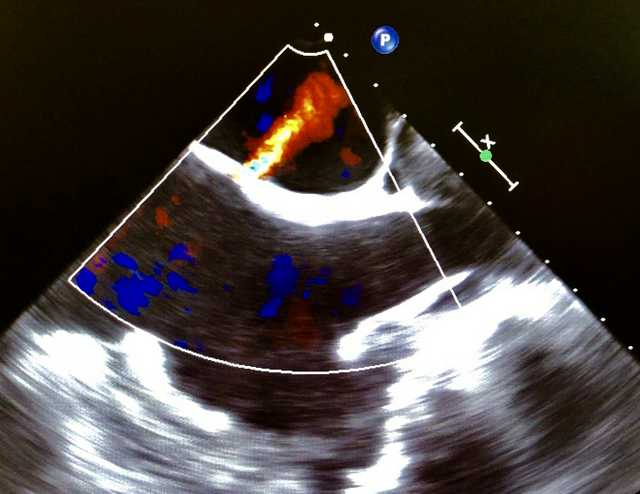
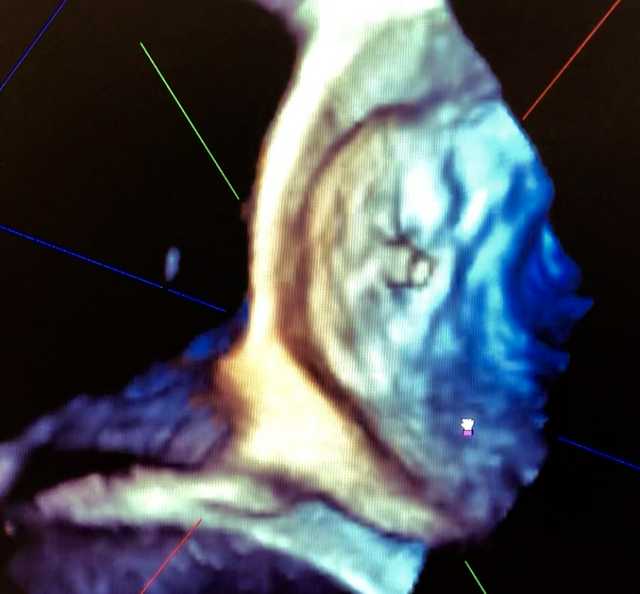
IVC is very telling of this patients right sided pressures.
Cryoablations run a significant risk of perforation so for those, we put an arterial line and second IV or piggyback off the cardiologist. Fortunately it doesn't happen often but when it does, we need to prepared. Remember the ASA ad. "where seconds count"
This is one of those times. Early detection and aggressive response are important to save the patient.
This is one of those times. Early detection and aggressive response are important to save the patient.
Academic center, very slow fellows/attendings with almost all get pre induction aline as requested by cardiologist and they still place a femoral sometimes.
aflutter on right side, usually no a-line
otherwise yes
otherwise yes
EP here... where I'm at Anesthesia will put in radial a-lines for all Afib (under general) and VT ablations. Most of our right sided stuff (flutter, most other SVTs, right sided PVCs) are done awake or with MAC. A-line decision not really driven by us, more dictated by what the Anesthesiologist there that day is comfortable with.
Academic center, very slow fellows/attendings with almost all get pre induction aline as requested by cardiologist and they still place a femoral sometimes.
Awake art lines for ablations? What’s the cardiologist reasoning for this?
Awake art lines for ablations? What’s the cardiologist reasoning for this?
Lot of them have crap hearts and get hypotensive quick on induction even if you're careful. There is also a distinct possibility of crashing right there on the table, away from the main ORs.
Lot of them have crap hearts and get hypotensive quick on induction even if you're careful. There is also a distinct possibility of crashing right there on the table, away from the main ORs.
This. I have had more than a few go asystole(no joke, for up to 5s) in cardiac lab, not in ablation but pace maker cases in a MAC case.
Advertisement - Members don't see this ad