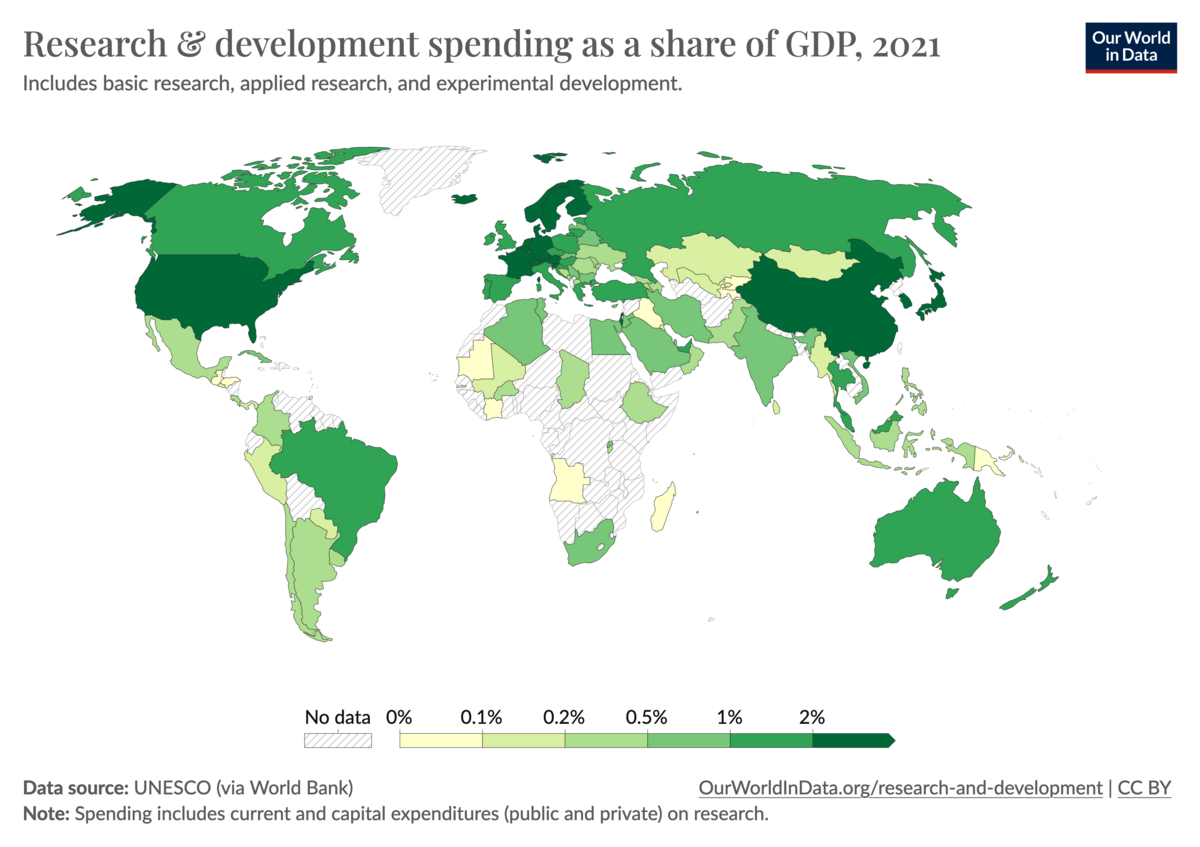
The page you yourself linked doesn't even support that assertion. The US not the top spender by any of the metrics: in absolute terms, it's China. As a percentage of GDP and per capita, it's Israel. As a percentage of GDP the US doesn't even make top 10 - ranking below Germany and a bit above Slovenia or Belgium. But anyway, I meant more generally willingness to fund public goods, including research but also education (US ranked 65), universal healthcare (unranked...), etc.
What you are failing to consider is that the program is very small, with few MD-PhD training spots nationally and limited capacity for schools to expand them. While the absolute investment may not be very large, the per capita investment is quite large; the cost to train each MD-PhD is somewhere between $500k-1m, split between the MSTP, F30/F31 grants, other NIH grants, state taxes (for state schools) and university endowments. The problem is not that it will break the NIH's bank, but that places are scarce and most applicants do not get a spot anywhere (
only about a third of applicants get accepted anywhere, out of a pool that is already heavily self-selected), so people who join the program without the intention of practicing medicine or doing research are taking spots from people who do.
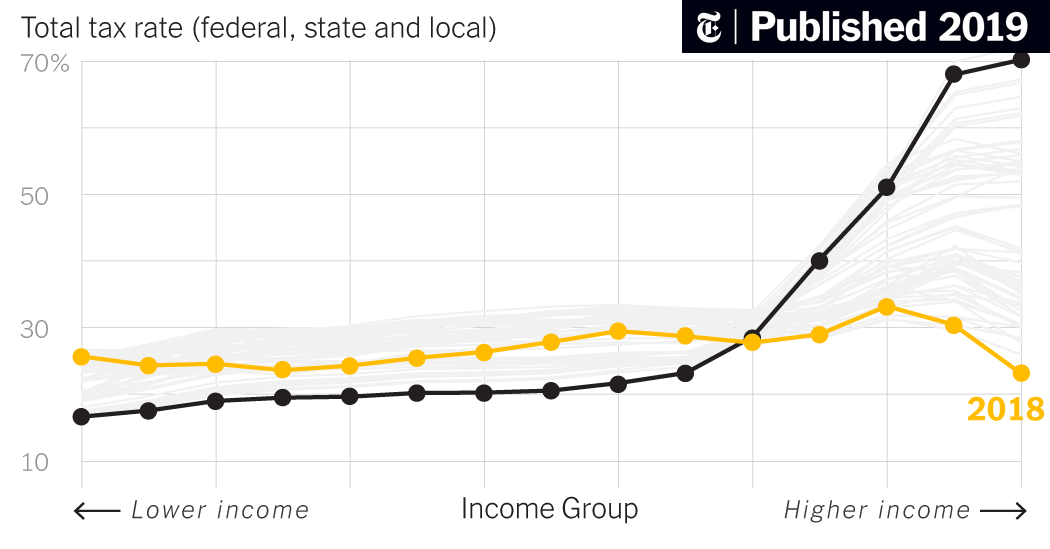
Ah yes, the Effective Altruism argument. The main barrier to funding public services is not lack of wealth creation but wealth inequality and in particular regressive taxation. The wealthiest Americans are paying less as a percentage of their income in taxes than the poorest; but we don't need to get into all of that here. The more pertinent point is, well by that logic, why do you need to accept public investment in order to do so? If your goal is to create wealth, and you believe doing so is virtuous because you will pay taxes that will go to services for poorer people, why not self-fund your way through med school, or work in industry straight out of undergrad, or for that matter work in finance?
"I suppose you could argue a private practice in X Y Z is not "research-related" enough...LOL but I think that's just a pretty sad argument" - I don't see what your problem is; obviously, becoming a full-time private practitioner is patently incongruous with that stated goal?
But I think this is a good opportunity to take a step back here: I specifically never said I thought the problem was MD-PhDs going into industry; indeed I believe there are valid reasons for an MD-PhD to go into industry. I said the problem is accepting the public investment in research that the MD-PhD represents with the goal of using it for wealth generation, whether that be in industry or in private practice.
An analogy that comes to mind is the investment that goes into military training - it is very expensive and gives the trainee very valuable skills, tuition-free. Naturally, this training comes with a service requirement to make sure the government and the public receive value from this investment (whether the investment in the military actually provides a public good is immaterial to my analogy). If they had wanted to at the inception of the program, I'm sure the NIH could have conditioned receiving MSTP funding on completing residency, or Peace Corps service, or some sort of postdoctoral scientific service requirement. I think the choice to make the funding "no strings attached" is an expression of good faith: the NIH is understanding that there are multiple definitions of a successful outcome when it comes to "undertak[ing] biomedical research and research-related careers," and also that life happens and people's goals at the end of a long training program may not be the same as the goals they had coming in, and doesn't want to tie someone down to a career they no longer wish to pursue.
I am of the belief that this good faith should be reciprocated. It is not some huge sacrifice to live on "only" $200k or $300k a year - without debt, this income is already enough to make you wealthy; why does it matter if it's not "as wealthy" as some private practitioner making $800k a year? When you apply, you have to explain your reasons for wanting to do an MD-PhD, and all programs are looking for candidates who express a desire to use the training for a research career. If you make that commitment without the intention of following through, you are deliberately misrepresenting yourself, to the detriment of other qualified candidates. This is not being "devious", it is taking advantage of a system deliberately designed to have few protections against being taken advantage of.