Advertisement - Members don't see this ad
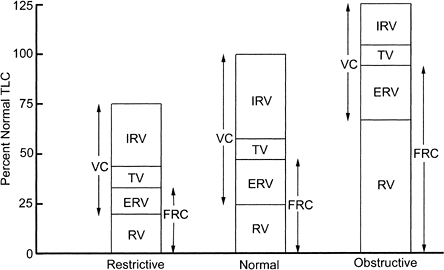
I'm having a bit trouble grasping the change in FRC in Obstructive Lung Disease. I always assumed that it would be increased given the air trapping that occurs in the lungs. But according to SUTS2 it is markedly decreased.
Is this because while the RV increases, the ERV decreases even more? Or is there some other reason?
Is this because while the RV increases, the ERV decreases even more? Or is there some other reason?