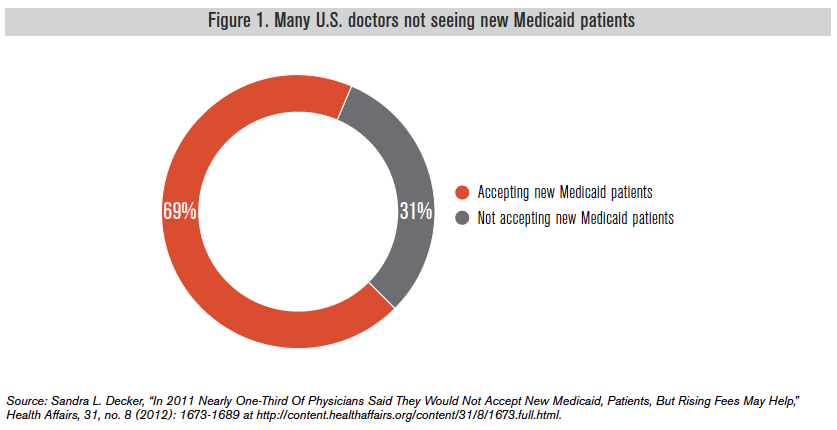
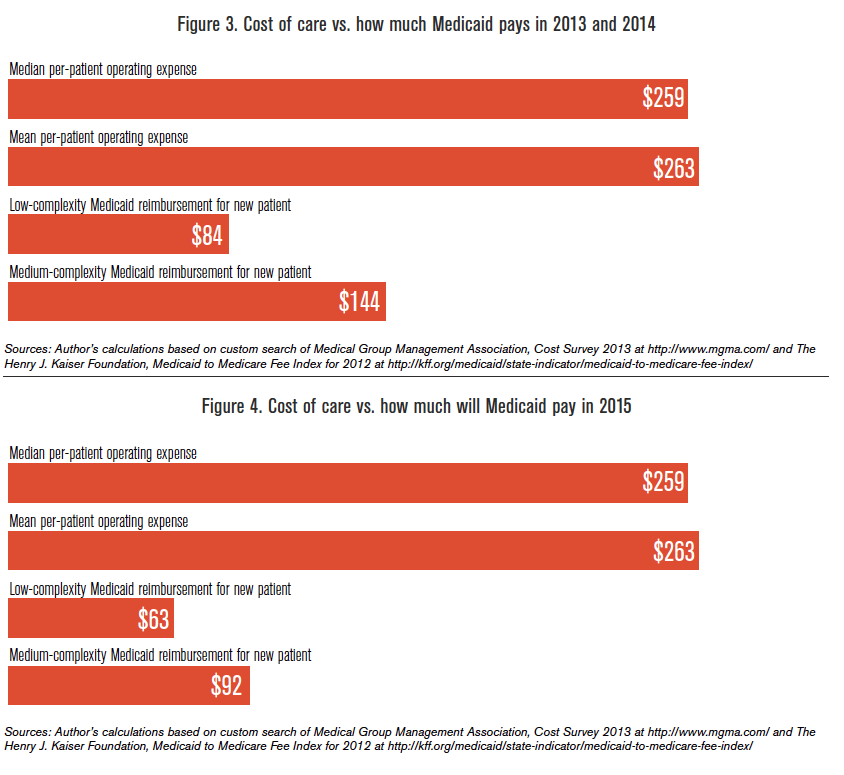
Reimbursement rates set by Medicaid?
Dermatologist have more cash payors and Orthopods more procedures? Is it also because both dermatologists and orthopods tend to see a higher New Visit to Established Visit ratio?
Differing CPT code mix and payor mix per RVU
OK, let's start with the basics
In this situation, Patient A sees a doctor (doesn't matter if it is a PCP, dermatologist, orthopod, rheumatologist, etc)
The doctor will see the patient, obtain the relevant HPI, ROS, PMH/PSH/FHx/SHx, PE, and come to a diagnosis and treatment plan. An outpatient E/M code is then used to bill insurance company depending on level of service (LOS) - which is predefined by CMS. You can't just go "well, I think this is a complex case so therefore I will bill as a level 5 comprehensive new patient visit" without appropriate supporting documentation.
If the PCP or dermatologist wrote:
This new patient is 65 yo M male with 2-week history of a severely, itchy red rash on his face, not improving with over-the-counter lotion. Patient is not taking any new medications.
Past medical history: Asthma
Social history: Negative for tobacco
Review of systems (ROS): Negative for new growths or fever
PE: patchy erythema accompanied by induration along the V2 distribution on right side of face, with grouped herpetiform vessicles apearing unilaterally
A/P: Herpez Zoster. Plan - treat zoster for symptoms and +/- antiviral
The above note contains 5 HPI points (detailed hx), 2 ROS, 2 PMSFHx, expanded-focused PE, and complex medical decision making (including writing Rx). For a new patient, you need all 3 "levels" (history, exam, medical decision making) to be in agreement to bill at that level, otherwise you bill at the lowest level that you documented. For return patients, you just need 2 out of 3. In this case, this note should be a new patient level 3 office visit (99203) because the exam component didn't meet the requirment for level 4 or 5 visit. So a doctor may submit a 99204 or 99205 code, but a good biller/coder (that the doctor hires) will catch this, and ask the doctor to resubmit as a 99203. If the doctor submits this as a 99205, and a year later gets audited, the auditor will not that the visit was "upcoded" and will penalize the doctor for this (the doctor will be accused of overcharging or overbilling Medicare and committing Medicare Fraud)
NOW the details of what constitute a new patient, what qualifies as a level 1, 2, 3, 4, 5 visits, etc are beyond the scope of medical students and it should NOT be something that at this level needs to be learned. The above is just a glimpse on what your preceptor is thinking when he enters a billing code during your outpatient rotation exposure (ie during family medicine, part of internal medicine, pediatrics, etc). As a resident, you should start to be familiar with this since you are seeing patients in your continuity clinic and starting to bill (albeit under your attending's name so ultimately your attending has final say) and should know this stuff once you are done with training since it will be your name (and liability) attached to each bill you submit.
Your personal income is basically Gross Income - Overhead. Like any other business, gross income is determined by how much you can collect (not necessarily bill). You bill in hopes that the insurer will pay what you bill (and not downcode your visit or deny the visit altogether even though you have already provided service). So when you see surveys and see the average family medicine income vs dermatology vs orthopedic spine vs pediatrics vs pulmonary vs GI - the same principle applies - income is Gross Income - overhead.
So what determines Gross Income? There's actually a complex formula developed by CMS that generates a physician fee schedule for physician services. Physician Services include Office Visits, Surgical Procedures, and Diagnostic/Therapeutic Services.
Each CPT code (whether diagnostic or procedure) is assigned a RVU (relative value unit), predetermined by CMS. RVU is usually determined by physician work (52%), practice expense (46%) and malpractice liability (2%). However it gets way more complicated based on where you work and type of setting that you work ... so the work done in a hospital outpatient setting in California may be reimbursed differently than the same work done in a rural Kentucky PCP's office (since it takes geolocation using GPCI, cost of practice, etc)
Now you submit your bill to insurance as a 99203 visit. (some insurance will still accept an outpatient consult 99243 instead of outpatient new patient visit, but a lot of commercial insurance followed CMS lead in rejecting outpatient consult codes). In 2014, a 99203 visit will generally be reimbursed $108 (1.42 RVU), BUT there are external factors that can affect that reimbursement rate (mainly where you practice since medicare does take region and cost of practice into consideration, whether you are participating in PQRS, meaningful use, if you're using EMR, etc). Usually insurance companies will reimburse based on a percentage of Medicare's prevailing rate, although for large health systems they can negotiate that rate (either higher or lower depending on market strength by either the health system OR insurer). A recent survey of doctors report that for 99203 visits, roughly 25% of physicians get reimbursed less than $75 for a 99203, about a third get between $75-$100 for a 99203, and 42% get reimbursed more than $100. According to the AMA, a 99203 visit should take 30 minutes.
So let's say the family medicine doctor sees 2 new patients in an hour, makes a diagnosis (and correctly finds the right ICD10 code), and submits 99203 codes for both patients. For that hour of work, the gross income should be $216 (for this example). A dermatologist who sees 2 new patients in an hour, submits the relevant ICD10 code, and bills 99203 codes will get reimbursed the same. An orthopedic surgeon who sees 2 new patients in his office will also submit the ICD10 codes and bill 99203 codes and get paid the same* (will discuss global payments later but in this case, new patient, no surgery yet). **I know my dermatology and orthopedic colleagues are laughing right now at the concept of seeing 2 new patients an hour.
So at the end of the hour, the family medicine doctor, dermatologist, and orthopedic surgeon have seen 2 patients, billed, and have generated $200 in gross income. Medicare/medicaid/Blues/Tricare/Aetna do not care if you're a harvard-trained dermatologist, or a small community hospital trained PCP and makes no such adjustments (a common misconception that some premeds have is that reimbursement is tied to prestige of training). They also don't care if you have $20k in student loans, or $350k in student loan.
But back to the original question:
So why are the incomes different at the end of the day/year?

")