- Joined
- Oct 23, 2005
- Messages
- 8,317
- Reaction score
- 6,059
- Points
- 7,396
- Attending Physician

SI (lateral branch) RFA works if you do a robust palisade technique, too bad it doesn’t get paid for.
ESIs for stenosis have poor evidence, but we’ll keep doing them.
MILD makes sense if there is a thick ligament. It may even help NFN at treated levels.
Intracept is a game changer.
We need to do a lot more sacroplasty. Beall will teach you how.
SIBone has serious issues, but there are several other SI fusion options.
Genicular RF may work better if we do more sites.
Si joints can look funny. You can use steroids in diagnostic injections to treat them.
Transitional vertebrae are common. They may hurt if type II or IV. They feel better if a Mayo radiologist injects them. If that doesn’t work, the evidence isn’t clear on what to do. Some have RFed them, they are sometimes resected.
SCS is the answer. What was the question?
Inject enough contrast to get to your target - video of delayed vascular uptake in a CTFESI was shown and was really interesting
I’m glad that intracept is a game changer, I just wished it paid better for non HOPD employed pain physician.
you know the sense that I got was that they were making a case that this procedure shouldn't be abandoned and we just need to review the MRI for potential vascular anomalies, enter the posterior foramen at a more shallow angle of approach, only use dex (and don't mix dex with local), and use digital subtraction imaging to make it as safe as possible.was any comment made why people are still doing CTFESI?
intracept apparently wont pay will for HOPD physician either.
Thanks. Bummed I couldn’t make it this year. Pretty sure I’ll be there next year.That’s a really good summary @cowboydoc
I’ll add:
Start making someone in your practice create templates based off the LCDs and keep them updated to make sure you get paid
Don’t submit bills for 26 epidurals on the same patient in a year or 51 RFA sites on a patient in one day
Vertiflex might work better than X stop but surgeons don’t like when local kyphosis affects sagittal balance
Inject enough contrast to get to your target - video of delayed vascular uptake in a CTFESI was shown and was really interesting
Probably best to avoid gad altogether in the epidural space regardless of approach
TFESIs have the best (although not great) evidence for LSS
Don’t miss spinal dural AVFs
Nice comments, they claimed the rct will be published soon, assuming it is positive.that chemical neurolysis for knee article is behind a firewall, but the summary is kind of a waste of time.
retrospective observational study. contacted by phone for follow up.
at least they used phenol, which one can still conceivably get (absolute alcohol too expensive for neurolysis)
Thanks for the updates. Can you say more about the Gad? I still will use for TFESI but have stopped for interlaminar. ThanksThat’s a really good summary @cowboydoc
I’ll add:
Start making someone in your practice create templates based off the LCDs and keep them updated to make sure you get paid
Don’t submit bills for 26 epidurals on the same patient in a year or 51 RFA sites on a patient in one day
Vertiflex might work better than X stop but surgeons don’t like when local kyphosis affects sagittal balance
Inject enough contrast to get to your target - video of delayed vascular uptake in a CTFESI was shown and was really interesting
Probably best to avoid gad altogether in the epidural space regardless of approach
TFESIs have the best (although not great) evidence for LSS
Don’t miss spinal dural AVFs
As little as 0.1ml has been implicated in encephalitis with IT administrationThanks for the updates. Can you say more about the Gad? I still will use for TFESI but have stopped for interlaminar. Thanks
Is that where you told your wife the chlamydia came fromA Chicago Handshake tastes like cunilingus with a Koala bear.
they showed some cases were you can get a root sleeve in the foramen and could potentially inject into it and be intrathecalThanks for the updates. Can you say more about the Gad? I still will use for TFESI but have stopped for interlaminar. Thanks
Why is it called a Chicago Handshake?Never put ketchup on a Chicago dog.
Italian hot beefs sweet and juicy are better than hot and dry.
The Aviary and London House are where the cool kids are for fun.
A Chicago Handshake tastes like cunilingus with a Koala bear.
If you can buy shares in a physician-owned hospital, you should.
If you can't control incentives people receive, you can't control their behavior.
Most of the dancers at Rick's are saving their money for college.
"They will never love you back."
I did too. Based on Dr. Usso's description, I thought it was political/sexual innuendo.Why is it called a Chicago Handshake?
In the Chicago drinking world, the Chicago Handshake is slang for a drink special involving a shot of Jeppson's Malört paired with an 'old-school' Midwestern beer, most typically Old Style Beer. Although Old Style originated in Wisconsin, it became Chicago's beer after crossing state lines in 1935.
Had to look it up.
Based on his reputation, so did I.I did too. Based on Dr. Usso's description, I thought it was political/sexual innuendo.
Office trials are lucrative re NaluPNS is still only for HOPD?
Whats the reimbursement and lead cost? ThanksOffice trials are lucrative re Nalu
I’d reach out to rep for office based trials.Whats the reimbursement and lead cost? Thanks
 www.nature.com
www.nature.com
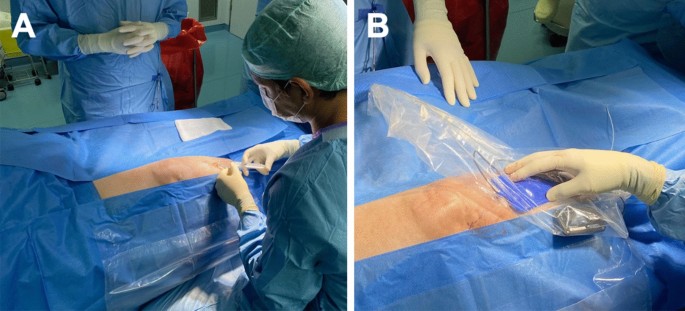
2/33 got infected. Study done by Neurosurgery departments. For OA knee.Peripheral nerve stimulation for chronic knee pain:
Any comments on this are welcome and appreciated, thanks.Peripheral nerve stimulation for the treatment of chronic knee pain - Scientific Reports
The average age of our population is increasing, resulting in a high incidence of chronic degenerative knee pathologies. Several treatment options, including surgical procedures are available to help mitigate these pathologies. However, the percentage of subjects with chronic post-surgical knee...
Thanks for the quick response, comments are appreciated, Authors from Germany, are they lying very often😉2/33 got infected. Study done by Neurosurgery departments. For OA knee.
6/33 did not benefit.
COI reports none, yet it reads like an advertisement in the conclusion/discussion.
Shady at best. Lying is much more likely.
I’m all in for doing 15 or so sites with two burns each for genicular.. with any luck I’ll soon be able to afford a new little tykes tricycle to commute with..SI (lateral branch) RFA works if you do a robust palisade technique, too bad it doesn’t get paid for.
ESIs for stenosis have poor evidence, but we’ll keep doing them.
MILD makes sense if there is a thick ligament. It may even help NFN at treated levels.
Intracept is a game changer.
We need to do a lot more sacroplasty. Beall will teach you how.
SIBone has serious issues, but there are several other SI fusion options.
Genicular RF may work better if we do more sites.
Si joints can look funny. You can use steroids in diagnostic injections to treat them.
Transitional vertebrae are common. They may hurt if type II or IV. They feel better if a Mayo radiologist injects them. If that doesn’t work, the evidence isn’t clear on what to do. Some have RFed them, they are sometimes resected.
SCS is the answer. What was the question?
so they really only "studied" the patients that had benefit.2/33 got infected. Study done by Neurosurgery departments. For OA knee.
6/33 did not benefit.
COI reports none, yet it reads like an advertisement in the conclusion/discussion.
Shady at best. Lying is much more likely.
A further notable limitation of our study is the absence of a control group, specifically patients who underwent TKA with standard post-operative care. This absence may introduce potential biases, as comparisons with standard care or other treatment options cannot be made. Future studies should consider including control groups to better elucidate the relative effectiveness of the treatment under investigation.
This week i talked to a guy in boston Edgar Ross, he was very positive about genicular nerve stim for post-surgical knee pain, he followed up patients for decades. Any comments on this? Thanks2/33 got infected. Study done by Neurosurgery departments. For OA knee.
6/33 did not benefit.
COI reports none, yet it reads like an advertisement in the conclusion/discussion.
Shady at best. Lying is much more likely.
Go see who pays him to spout this nonsense. Bet you sprintpns and Medtronic are on the list of many.This week i talked to a guy in boston Edgar Ross, he was very positive about genicular nerve stim for post-surgical knee pain, he followed up patients for decades. Any comments on this? Thanks
I’m skeptical of stim for knee pain but that type of academic practice is gonna see a way different patient population than most on this forum.
Not here to pick a fight. Delusional and spouting nonsense is not Ed.