If a patient cannot afford crown lengthening surgery and he has deep subgingival amalgam fillings mesially and distally, then is it ok to leave them on the crown margin? A crown that fits is obviously preferable than a crown that doesn't fit and there's a higher likelihood of a poorly prepped margin and a poorly captured margin if the margin is very deep. In addition, a crown margin that's too deep could violate the biologic width and cause the patient problems afterwards. I know it's not ideal but under these circumstances, is it ok to leave the amalgam (or composite) filling on the crown margin?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Is it below the standard of care to leave amalgam or composite on a crown margin?
- Thread starter Apexica
- Start date

- Joined
- Jan 26, 2015
- Messages
- 2,691
- Reaction score
- 7,654
Research “deep margin elevation.”
Big Hoss
Big Hoss
I've seen deep margin elevation mostly with Class 2 restorations but if it's done on a crown, there's going to be composite (or similar) material on the margin. So are you saying it's ok to leave composite or amalgam on a crown margin? Because I've heard some dentists say that you shouldn't.Research “deep margin elevation.”
Big Hoss
- Joined
- Jan 26, 2015
- Messages
- 2,691
- Reaction score
- 7,654
Do your research. Apply what you think is best to this clinical situation. Discuss options with the patient. You’re the dentist.So are you saying it's ok to leave composite or amalgam on a crown margin? Because I've heard some dentists say that you shouldn't.
Big Hoss
- Joined
- Mar 4, 2008
- Messages
- 196
- Reaction score
- 153
Deep Margin Elevation: A Literature Review
A conservative approach for restoring deep proximal lesions is to apply an increment of composite resin over the preexisting cervical margin to relocate it coronally, the so-called “deep margin elevation” (DME). A literature search for research articles referring to DME published from January...
Abstract
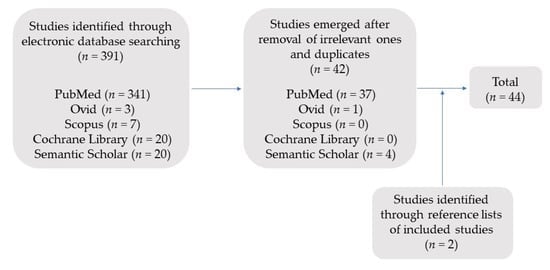
A conservative approach for restoring deep proximal lesions is to apply an increment of composite resin over the preexisting cervical margin to relocate it coronally, the so-called “deep margin elevation” (DME). A literature search for research articles referring to DME published from January 1998 until November 2021 was conducted using MEDLINE (PubMed), Ovid, Scopus, Cochrane Library and Semantic Scholar databases applying preset inclusion and exclusion criteria. Elevation material and adhesive system employed for luting seem to be significant factors concerning the marginal adaptation of the restoration. This technique does not affect bond strength, fatigue behavior, fracture resistance, failure pattern or repairability. DME and subgingival restorations are compatible with periodontal health, given that they are well-polished and refined. The available literature is limited mainly to in vitro studies. Therefore, randomized clinical trials with extended follow-up periods are necessary to clarify all aspects of the technique and ascertain its validity in clinical practice. For the time being, DME should be applied with caution respecting three criteria: capability of field isolation, the perfect seal of the cervical margin provided by the matrix, and no invasion of the connective compartment of biological width.
So what I'm getting from these articles on DME is that yes it's ok to have filling material on the crown margin and that no, it's not below the standard of care. My concern of having a restoration material on the margin is that they eventually wear due to the occlusal forces placed on the crown and this could compromise the margin in the future.
So if it's ok to have composite on the crown margin, then wouldn't you prefer to use a stronger material like amalgam? At least amalgam lasts significantly longer than composite. Some sources even have amalgam matching the lifespan of a ceramic crown. So if the patient has a deep amalgam MOD and there is no decay, when prepping it for a crown is it ok to just leave some of the amalgam on the margins instead of removing it all and then doing DME? After all, the margin is already elevated by the existing amalgam.
So if it's ok to have composite on the crown margin, then wouldn't you prefer to use a stronger material like amalgam? At least amalgam lasts significantly longer than composite. Some sources even have amalgam matching the lifespan of a ceramic crown. So if the patient has a deep amalgam MOD and there is no decay, when prepping it for a crown is it ok to just leave some of the amalgam on the margins instead of removing it all and then doing DME? After all, the margin is already elevated by the existing amalgam.
- Joined
- Mar 4, 2008
- Messages
- 196
- Reaction score
- 153
Yes amalgam is ok and preferred in some articles iircSo what I'm getting from these articles on DME is that yes it's ok to have filling material on the crown margin and that no, it's not below the standard of care. My concern of having a restoration material on the margin is that they eventually wear due to the occlusal forces placed on the crown and this could compromise the margin in the future.
So if it's ok to have composite on the crown margin, then wouldn't you prefer to use a stronger material like amalgam? At least amalgam lasts significantly longer than composite. Some sources even have amalgam matching the lifespan of a ceramic crown. So if the patient has a deep amalgam MOD and there is no decay, when prepping it for a crown is it ok to just leave some of the amalgam on the margins instead of removing it all and then doing DME? After all, the margin is already elevated by the existing amalgam.
Leaving an old amalgam can be iffy because those MOD boxes sometimes hide a crack, or caries.
- Joined
- Dec 1, 2000
- Messages
- 2,938
- Reaction score
- 658
Would you rather the patient have 1 or 2 interfaces between tooth structure and/or any remaining pre-existing restorative materials and your new crown to maintain and clean?
The reality is even if the patient can't afford formal crown lengthening surgery, if you prep a subgingival margin to "clean" natural tooth structure, and can get a good impression of that margin and seat and cement a well fitting crown, the basic concept of biologic width will, over time, in essence naturally handle that crown lengthening for you and your patient. Is it ideal? Nope. Does it work from time to time in my own patient population over the last 20+ year? Yes
Sometimes real life patient management situations and the "ideal" treatment plan will differ. And in reality in a clinical situation like you mentioned, do you think the patient will be better off from a longterm functional standpoint, if you have determined that the patient's tooth should be crowned, but they can't afford the crown lengthening if you in essence with your prep do some crown lengthening which then the natural biological width process will "finish" for you, or leave the patient with whatever assortment of direct restorative materials you may use is in that tooth without a crown on it?
Whne it comes to treatment planning, the majority of the time you will "think inside the box" and stay within the treatment planning concepts you have been taught, however, you will certainly encounter situations in practice over time where you will have to "think outside the box" and treatment plan in a different way that what you were taught. Inform the patient, have the conversation with them of the pros and cons, document things, and go for it from time to time. You do have to think on your own and not just follow a rigid protocol all the time just because Professor X in the prosth department rigidly gave you a procedural list that you have to follow to get all of your prosth credits for graduation.
The reality is even if the patient can't afford formal crown lengthening surgery, if you prep a subgingival margin to "clean" natural tooth structure, and can get a good impression of that margin and seat and cement a well fitting crown, the basic concept of biologic width will, over time, in essence naturally handle that crown lengthening for you and your patient. Is it ideal? Nope. Does it work from time to time in my own patient population over the last 20+ year? Yes
Sometimes real life patient management situations and the "ideal" treatment plan will differ. And in reality in a clinical situation like you mentioned, do you think the patient will be better off from a longterm functional standpoint, if you have determined that the patient's tooth should be crowned, but they can't afford the crown lengthening if you in essence with your prep do some crown lengthening which then the natural biological width process will "finish" for you, or leave the patient with whatever assortment of direct restorative materials you may use is in that tooth without a crown on it?
Whne it comes to treatment planning, the majority of the time you will "think inside the box" and stay within the treatment planning concepts you have been taught, however, you will certainly encounter situations in practice over time where you will have to "think outside the box" and treatment plan in a different way that what you were taught. Inform the patient, have the conversation with them of the pros and cons, document things, and go for it from time to time. You do have to think on your own and not just follow a rigid protocol all the time just because Professor X in the prosth department rigidly gave you a procedural list that you have to follow to get all of your prosth credits for graduation.
- Joined
- Apr 13, 2020
- Messages
- 513
- Reaction score
- 636
Deep Margin Elevation: A Literature Review
A conservative approach for restoring deep proximal lesions is to apply an increment of composite resin over the preexisting cervical margin to relocate it coronally, the so-called “deep margin elevation” (DME). A literature search for research articles referring to DME published from January...www.mdpi.com
Abstract
A conservative approach for restoring deep proximal lesions is to apply an increment of composite resin over the preexisting cervical margin to relocate it coronally, the so-called “deep margin elevation” (DME). A literature search for research articles referring to DME published from January 1998 until November 2021 was conducted using MEDLINE (PubMed), Ovid, Scopus, Cochrane Library and Semantic Scholar databases applying preset inclusion and exclusion criteria. Elevation material and adhesive system employed for luting seem to be significant factors concerning the marginal adaptation of the restoration. This technique does not affect bond strength, fatigue behavior, fracture resistance, failure pattern or repairability. DME and subgingival restorations are compatible with periodontal health, given that they are well-polished and refined. The available literature is limited mainly to in vitro studies. Therefore, randomized clinical trials with extended follow-up periods are necessary to clarify all aspects of the technique and ascertain its validity in clinical practice. For the time being, DME should be applied with caution respecting three criteria: capability of field isolation, the perfect seal of the cervical margin provided by the matrix, and no invasion of the connective compartment of biological width.
From my 25 years of observations, the success rate is directly proportional to the patient's caries risk levels. I followed a handful of cases like this done by other providers (I never applied this technique) for a few years and had to do some marginal repair on half of them. If you have the luxury of seeing this patient for many years prior to this case, or if you have access to previous x-rays to gauge the caries risks, it may be more predictable. Be mindful of potential Board or Legal actions and definitely document effectively.
I'm less concerned about legal actions because if something went south I would 100% refund the patient or re-do the procedure for free (and perhaps even pay for the crown lengthening). I'm more concerned if this is something that a state Board would regard as below the standard of care. That's why it's the title of this thread. Say for instance a dentist uses 10 carpules of lidocaine with epinephrine on a 7 year old child or if a dentist places a mandibular implant without doing the proper imaging (CT scan, etc). Those would be considered below the standard of care. From what I'm getting from this thread and from the articles is that leaving filling material on a crown margin is something that some dentists do and some dentists don't. To me that doesn't seem like something that is below the standard of care but a treatment option that is up for debate. Does anyone disagree with that and think that leaving filling material on a crown margin is below the standard of care? So far in this thread, no one believes that it is...Be mindful of potential Board or Legal actions and definitely document effectively.
- Joined
- Apr 13, 2020
- Messages
- 513
- Reaction score
- 636
Your concerns are very valid. I have an ex-superviser who is or maybe was a member of my state Board. I will try to contact him about this. We will always encounter cases that are far from "text book" and like @DrJeff mentioned, we may have to think "outside the box" of course being in the best interest of the patient. Having delt with my state Board before, they are very reasonable and will clear you with good documentation. I think this topic can be "gray." If the clinician prepped the margins above the solid filling material, explained and documented the reasoning, any state Board will not consider it "below standard of care" and clear you.I'm less concerned about legal actions because if something went south I would 100% refund the patient or re-do the procedure for free (and perhaps even pay for the crown lengthening). I'm more concerned if this is something that a state Board would regard as below the standard of care. That's why it's the title of this thread. Say for instance a dentist uses 10 carpules of lidocaine with epinephrine on a 7 year old child or if a dentist places a mandibular implant without doing the proper imaging (CT scan, etc). Those would be considered below the standard of care. From what I'm getting from this thread and from the articles is that leaving filling material on a crown margin is something that some dentists do and some dentists don't. To me that doesn't seem like something that is below the standard of care but a treatment option that is up for debate. Does anyone disagree with that and think that leaving filling material on a crown margin is below the standard of care? So far in this thread, no one believes that it is...
- Joined
- Aug 28, 2008
- Messages
- 240
- Reaction score
- 163
Every time I remove an old amalgam I think to myself "man there is more caries under this thing than I thought there would be" and then I immediately remind myself that I should adjust(again) how I think about recurrent caries on amalgam restorations. In my practice of dentistry, if I find a reason to replace an older restoration for any reason (car, fracture, cuspal coverage, etc), if I didn't place it myself, I do everything possible to remove it all. If I didn't lay eyes on the tooth structure underneath, I don't know what's there and I am trusting that it was at one point clean and sealed. I think trying to avoid crown lengthening is like trying to avoid a root canal. Either you get all the car or you don't. If you worry too much about missing the pulp or the biologic width, what are you potentially leaving behind? You touch the tooth, you own what you leave behind when you are done.
Now, you placing a new restoration yourself and then doing a margin elevation for your new crown is a completely different clinical situation and can be an appropriate tx modality.
Now, you placing a new restoration yourself and then doing a margin elevation for your new crown is a completely different clinical situation and can be an appropriate tx modality.
- Joined
- Apr 13, 2020
- Messages
- 513
- Reaction score
- 636
I was fortunate to get a hold of my ex-supervisor who is still a member of my state Board. Along with other topics, he had mentioned,
"This is very interesting, and I tend to agree with you. If caries risk is high you might not even want to do a crown. I’m not speaking for the Board here, this is my opinion. If you explain the procedure to the patient and document appropriately most likely the Board would understand the reasoning for deviating from standard. Documentation should include reason (financial in this case), PARQ, and emphasis on the possible adverse outcomes explained to the patient. You can even do a consent form for the patient to sign if you want to be better protected. Of course, the procedure has to be done well. If the materials used are not properly sealing tooth structure and there are overhangs or gaps you might still be liable in the event of a complaint."
"This is very interesting, and I tend to agree with you. If caries risk is high you might not even want to do a crown. I’m not speaking for the Board here, this is my opinion. If you explain the procedure to the patient and document appropriately most likely the Board would understand the reasoning for deviating from standard. Documentation should include reason (financial in this case), PARQ, and emphasis on the possible adverse outcomes explained to the patient. You can even do a consent form for the patient to sign if you want to be better protected. Of course, the procedure has to be done well. If the materials used are not properly sealing tooth structure and there are overhangs or gaps you might still be liable in the event of a complaint."
Where can I find literature describing what the standard of care is? What about research supporting DME?I was fortunate to get a hold of my ex-supervisor who is still a member of my state Board. Along with other topics, he had mentioned,
"This is very interesting, and I tend to agree with you. If caries risk is high you might not even want to do a crown. I’m not speaking for the Board here, this is my opinion. If you explain the procedure to the patient and document appropriately most likely the Board would understand the reasoning for deviating from standard. Documentation should include reason (financial in this case), PARQ, and emphasis on the possible adverse outcomes explained to the patient. You can even do a consent form for the patient to sign if you want to be better protected. Of course, the procedure has to be done well. If the materials used are not properly sealing tooth structure and there are overhangs or gaps you might still be liable in the event of a complaint."
I think everyone is in agreement that more healthy tooth structure is better, but clinical dentistry isn’t so cut and dry. I don’t want to remove every tooth that doesn’t meet the most ideal crown conditions because tooth replacement options also have risks. CL has disadvantages and can expose furcation areas or affect adjacent teeth, so I think DME has its place.
Last edited:
- Joined
- Dec 1, 2000
- Messages
- 2,938
- Reaction score
- 658
The reality is that EVERYTHING we do as clinicians has some degree of risk to it, and how we learn to manage that degree of risk and effectively communicate it to our patients, is paramount to what we do, and likely why AI will never fully replace us, as in the future. Not everything is always going to be a cut and dry situationWhere can I find literature describing what the standard of care is? What about research supporting DME?
I think everyone is in agreement that more healthy tooth structure is better, but clinical dentistry isn’t so cut and dry. I don’t want to remove every tooth that doesn’t meet the most ideal crown conditions because tooth replacement options also have risks. CL has disadvantages and can expose furcation areas or affect adjacent teeth, so I think DME has its place.
- Joined
- May 6, 2018
- Messages
- 1,098
- Reaction score
- 2,329
In a lawsuit the “standard of care” is not concrete. You can’t use evidence or literature to back it up. It’s two clinicians on either side making the argument verbally.Where can I find literature describing what the standard of care is?
Last edited:
carabelliscusp
Full Member
- Joined
- Oct 27, 2022
- Messages
- 188
- Reaction score
- 129
In a lawsuit the “standard of care” is poor concrete. You can’t use evidence or literature to back it up. It’s two clinicians on either side making the argument verbally.
Surprising to hear knowing how its drilled into us D student's heads
Can you elaborate on how literature cannot be used to support clinical decisions in a lawsuit? That is interesting to me and I did not know that.In a lawsuit the “standard of care” is not concrete. You can’t use evidence or literature to back it up. It’s two clinicians on either side making the argument verbally.
- Joined
- Dec 7, 2017
- Messages
- 1,312
- Reaction score
- 1,911
You can use it but he is just saying you can't rely on that as strong evidence as a lawyer and clinician can find other literature for the opposing view. There are many things in dentistry that are as concrete as rubber dam for endoCan you elaborate on how literature cannot be used to support clinical decisions in a lawsuit? That is interesting to me and I did not know that.
It’s probably because the legal profession has little to do with what is true.Surprising to hear knowing how its drilled into us D student's heads
- Joined
- May 6, 2018
- Messages
- 1,098
- Reaction score
- 2,329
I don’t even think you’re allowed to use literature. At all. “Standard of care” arguments are entirely oral and can’t use outside information or support. It’s supposed to be whatever is “universally obvious” to the field based on expert opinion. It’s very inconcrete. At least that’s how they describe it at OMSNIC lectures. I’ve never been involved in a lawsuit myself.You can use it but he is just saying you can't rely on that as strong evidence as a lawyer and clinician can find other literature for the opposing view. There are many things in dentistry that are as concrete as rubber dam for endo
- Joined
- Apr 26, 2014
- Messages
- 120
- Reaction score
- 119
I would argue yes it would be considered below the standard of care to leave old restorative material on the margin, especially if the only reason is the margin would be "very deep". I also would argue that deep margin elevation (which is different than leaving an old filling behind at the margin) could be considered within the standard of care.
Consider the septocaine/paresthesia controversy: I don't think the literature supports the idea that septocaine is linked to a higher risk of paresthesia, but in a trial, the plaintiff's attorneys would be able to find an "expert witness" who will say that the link between septocaine and paresthesia is known and then a jury (of non-dental people) will hear that and immediately conclude the dentist made a mistake.
Consider the septocaine/paresthesia controversy: I don't think the literature supports the idea that septocaine is linked to a higher risk of paresthesia, but in a trial, the plaintiff's attorneys would be able to find an "expert witness" who will say that the link between septocaine and paresthesia is known and then a jury (of non-dental people) will hear that and immediately conclude the dentist made a mistake.
Similar threads
- Replies
- 4
- Views
- 662
- Replies
- 0
- Views
- 462