Advertisement - Members don't see this ad
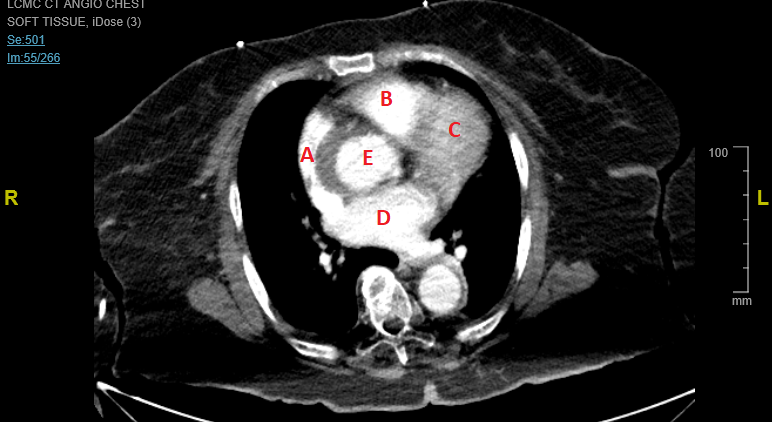
no so so far off. Look at the depth markers on the side (each dot is 1cm)Not showing up as a clip for me. But I see a hyperechoic circle that is maybe a PA catheter balloon or a cannula of sorts (ECMO vs bypass)?