- Joined
- Apr 19, 2016
- Messages
- 258
- Reaction score
- 839
Thank you to the authors for putting this together.
Big shout out to the Chairs who doubled residency spots over the same time and all the programs that SOAPed this year. Bright futures abound.

This is all the more annoying when you read the rationales given by CMS for the RO-APM. In summary, the reasoning for RO-APM in 2023 is: "IMRT cost us [CMS] a hell of a lot of money... between 2003 and 2009."
Thank you to the authors for putting this together.
Big shout out to the Chairs who doubled residency spots over the same time and all the programs that SOAPed this year. Bright futures abound.
Not having good lobbyists as compared to big pharma wouldn't flyThis is all the more annoying when you read the rationales given by CMS for the RO-APM. In summary, the reasoning for RO-APM in 2023 is: "IMRT cost us [CMS] a hell of a lot of money... between 2003 and 2009."
I just don’t get how:CMS Releases 2023 MPFS and HOPPS Final Rules: Payment cuts continue,
G codes face future scrutiny
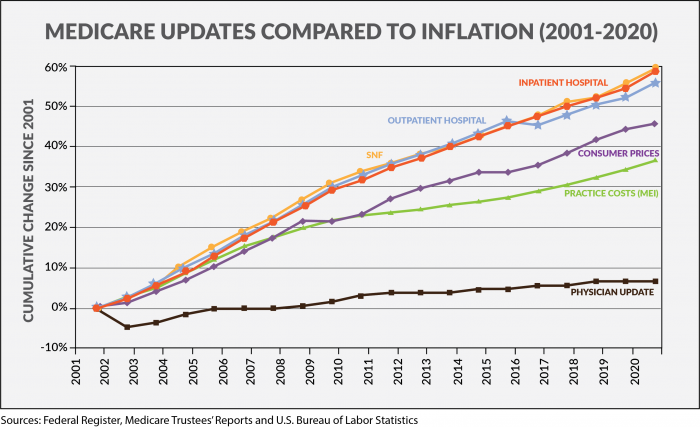
This evening, the Centers for Medicare and Medicaid Services (CMS) released the 2023 Medicare Physician Fee Schedule and Hospital Outpatient Prospective Payment System final rules, with cuts of 4% to radiation oncology due to reductions to the conversion factor and the second year of the clinical labor price update, which shifts resources from specialties to primary care services. Additionally, CMS notes in the MPFS that it is reviewing the current payment policy related to the conventional treatment delivery, IMRT and IGRT “G” codes, which could result in additional payment cuts in future rulemaking. ASTRO remains concerned that the continued payment cuts to radiation therapy services will impact access to care close to home. ASTRO and aligned stakeholders are actively lobbying Congress to address planned payment cuts by year end.
Please contact your member of Congress to oppose Medicare cuts. Additional MPFS and HOPPS analysis of specific code level impact and detailed summaries of both rules will be issued in the coming days.
I just don’t get how:
Cancer incidence is falling
RT utilization is falling
Long-course radiotherapy is disappearing
RT reimbursement is in a decade long free fall
But radiation oncologist numbers keep expanding. And they’re all getting hired!
It really messes with my desire to make sense of the universe.

Why I still can’t fathom any good medical student choosing rad onc lest one becomes one’s own cautionary tale about economics, and musical chairs.The music ends at some point.
Ha. Well we now have a pretty good long stretch where some very negative headwinds seem TO HAVE MATTERED ZERO in terms of the rad onc job market. Getting to the point that should I believe these lying lies of validated, published statistics and the lying liars who tell them… or twitter and my eyes.A 4% cut in this inflationary environment is more like a functional 12 or 15% cut in one year. But #radonc twitter tells me the future is bright, even KO says its true!
Takes roughly 20 years at negative 15% "compound interest" to hit a ~$25K annual salary if initially making $500K.Inflation 9% year over year. Public and government can't think because of poor education and rewarding of bad decision making. Want inflation relief checks. That will fix it.
Rad onc reimbursement down 4%.
15% pay decreases every year going forward.
Can somebody do the math and figure out when we will be making minimum wage in 2009 dollars? I would but my attention span is fried from smartphones just like the rest of the population.
Takes roughly 20 years at negative 15% "compound interest" to hit a ~$25K annual salary if initially making $500K.
Long row to hoe!
Inflation 9% year over year. Public and government can't think because of poor education and rewarding of bad decision making. Want inflation relief checks. That will fix it.
Rad onc reimbursement down 4%.
15% pay decreases every year going forward.
Can somebody do the math and figure out when we will be making minimum wage in 2009 dollars? I would but my attention span is fried from smartphones just like the rest of the population.
The old wise doctors when I first started out would always tell me “You will never again make as much money as you did today.” Wise indeed!Dirty secret: If everyone's wage went up the same rate as inflation (including all jobs, not just radonc), then we would never be able to leave the inflationary spiral.
Loss of purchasing power is better than loss of an entire country, which is what happens when hyperinflation begins. In addition, if the US doesn't protect its unique position as the issuer of the world's reserve currency, we will lose it and quickly understand what incredible benefits it brings.
We're all in this together, unfortunately. Does not excuse cuts in reimbursement, however, but I don't think we should at all expect them to keep up with the current inflation rate.
No, I agree with you. That was my point with the joke about inflation relief checks.Dirty secret: If everyone's wage went up the same rate as inflation (including all jobs, not just radonc), then we would never be able to leave the inflationary spiral.
Loss of purchasing power is better than loss of an entire country, which is what happens when hyperinflation begins. In addition, if the US doesn't protect its unique position as the issuer of the world's reserve currency, we will lose it and quickly understand what incredible benefits it brings.
We're all in this together, unfortunately. Does not excuse cuts in reimbursement, however, but I don't think we should at all expect them to keep up with the current inflation rate.
I'm guessing you made at least double in inflation-adjusted dollars. I know someone who was making about quadruple in NON inflation adjusted dollars in the early 00s compared to what I was making when I started a few years ago (and that was in the upper half of MGMA too!)The old wise doctors when I first started out would always tell me “You will never again make as much money as you did today.” Wise indeed!
Inflation hits everyone differently.... Someone renting a house with a gas guzzling SUV is feeling it a lot differently than the tree hugger running whole house solar on a house they've owned for awhile with a cheap mortgage, driving a Tesla and eating from their veggie garden etcNo, I agree with you. That was my point with the joke about inflation relief checks.
Inflation is a result an oversupply of money. Fixing that requires making money harder to come by, which is politically unpopular when people are competing for votes.
Real inflation is probably in the 15-20% range over the past year.
Last guy presided over the largest increase in money supply in recent history, of that I am sure."Inflation is always and everywhere a monetary phenomenon"
Uncle Milty
Old Joe says he is not in charge anymore but I am not so sure
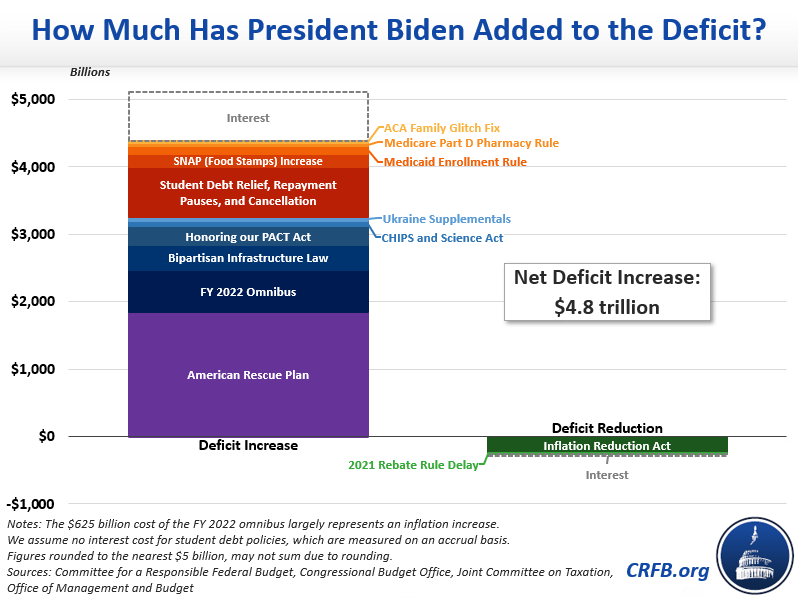
My observation is not partisan. Simple economics.Last guy presided over the largest increase in money supply in recent history, of that I am sure.
This has to go on Twitter.View attachment 361652
Well, this is interesting.
Are the rest of us taking a haircut to pay for raises for the elite?
WTF?View attachment 361652
Well, this is interesting.
Are the rest of us taking a haircut to pay for raises for the elite?

 communityoncology.org
communityoncology.org
That was 2020.. blowing it out of the water nowLast guy presided over the largest increase in money supply in recent history, of that I am sure.
View attachment 361652
Well, this is interesting.
Are the rest of us taking a haircut to pay for raises for the elite?
The field continues to circle the drain/toilet. The “leaders” are in their own world. The sycophant rasputin boot licking throne sniffers continue to tell the emperor he looks great despite no clothes. The worst isn't here yet.
You better believe it! Take it to the bank! Cha-ching.Can’t wait for that new ASTRO APM proposal to hit the market! Oh I’m sure protons and big RO will be spared.
You better believe it! Take it to the bank!
holy crapView attachment 361652
Well, this is interesting.
Are the rest of us taking a haircut to pay for raises for the elite?
holy crap
simul, please light em up.
He also said “think of how stupid the average person is, and realize half of them are stupider than that”. The field is “led” by people who matched when any warm body could walk into the field. Now think about the average bufoon “leader” and now realize half of them are stupider than that!Been going on for ages. This is why they can afford to poo poo community practice. They’ll always get a raise and you won’t.
As George Carlin used to say: it’s a big club and you ain’t in it!
holy crap
simul, please light em up.
When these giant institutions have people on staff that endless and breathless virtue signal and publish on this and that equity thing of the moment, it all comes off as just being extremely hypocritical. Usually the response will end up being, "well I know so and so and they are just so fantastic and care so much." It all reminds me of "green washing" in the esg space.
To think that Aileen chen and ben smith were allowed to give input into the adoption of the apm! Almost worse than Iran being on the UN women's rights council.Just one additional FU to community rad onc.
I’ve never met a group of weirdos so committed to killing their field or have such contempt for private practice than RO man.
MUCH MUCH easier to treat indigent patients in private practice. Very hard when I was at non-profit hospital based positions. Then, I got to this for-profit system. Now, interestingly, we were more community oriented and understanding about this population and can figure things out for struggling patients.I think, deep down, they know. They have to. They see the makeup of their patient populations. They know they're not treating that many minorities or impoverished patients. If they don't know they're perpetuating a system of inequity, they're willfully putting their heads in the sand to avoid having to deal with it.
My patients are of non-white majority and I have a two patients on treatment right now who are minorities who I am treating for free. It makes me feel good to not have to virtue signal, as I can allow my actions to speak for themselves, and it makes me feel good to help those who didn't have anywhere else to go.
Love to see it and 100% commend you and your practice for doing it.I think, deep down, they know. They have to. They see the makeup of their patient populations. They know they're not treating that many minorities or impoverished patients. If they don't know they're perpetuating a system of inequity, they're willfully putting their heads in the sand to avoid having to deal with it.
My patients are of non-white majority and I have a two patients on treatment right now who are minorities who I am treating for free. It makes me feel good to not have to virtue signal, as I can allow my actions to speak for themselves, and it makes me feel good to help those who didn't have anywhere else to go.
Love to see it and 100% commend you and your practice for doing it.
Curious though -- how do you decide who you're gonna help? Is there a formal program in place?
How does that work on the MO side? Free drug? I guess most of the concurrent regimens are generic anywaysYep, we have a formalized process for patients without insurance. We look into their financial information and charge only what they can afford. If they can't afford anything then we can write off the entire treatment.
It's simply a smart business choice. You want your referrings to think "I'll send this patient to OTN's practice, as I know no matter what he's going to make sure they're treated." I don't want referrings to ever have to think about who the patient's payor is and whether we will be able to treat. Gotta grease the slide as much as possible to get consults in.
How does that work on the MO side? Free drug? I guess most of the concurrent regimens are generic anyways
Pps exemption also applies to sattelites within 30 miles, but this has been challenged by some of the centers who apply it to all satellites.Do I understand correctly that the way the PPS exemption works, is they get paid for their expenses? Doesn't that design encourage these centers to be wasteful? Is the difference between these centers how much excess spending it takes to treat a patient?
Edited for phrasing
Pps exemption also applies to sattelites within 30 miles, but this has been challenged by some of the centers who apply it to all satellites.
When these giant institutions have people on staff that endless and breathless virtue signal and publish on this and that equity thing of the moment, it all comes off as just being extremely hypocritical. Usually the response will end up being, "well I know so and so and they are just so fantastic and care so much." It all reminds me of "green washing" in the esg space.
