
- Joined
- Nov 21, 1998
- Messages
- 12,566
- Reaction score
- 6,962
Inches, Centimeters, and Yards: Overlooked Definition... : The Clinical Journal of Pain
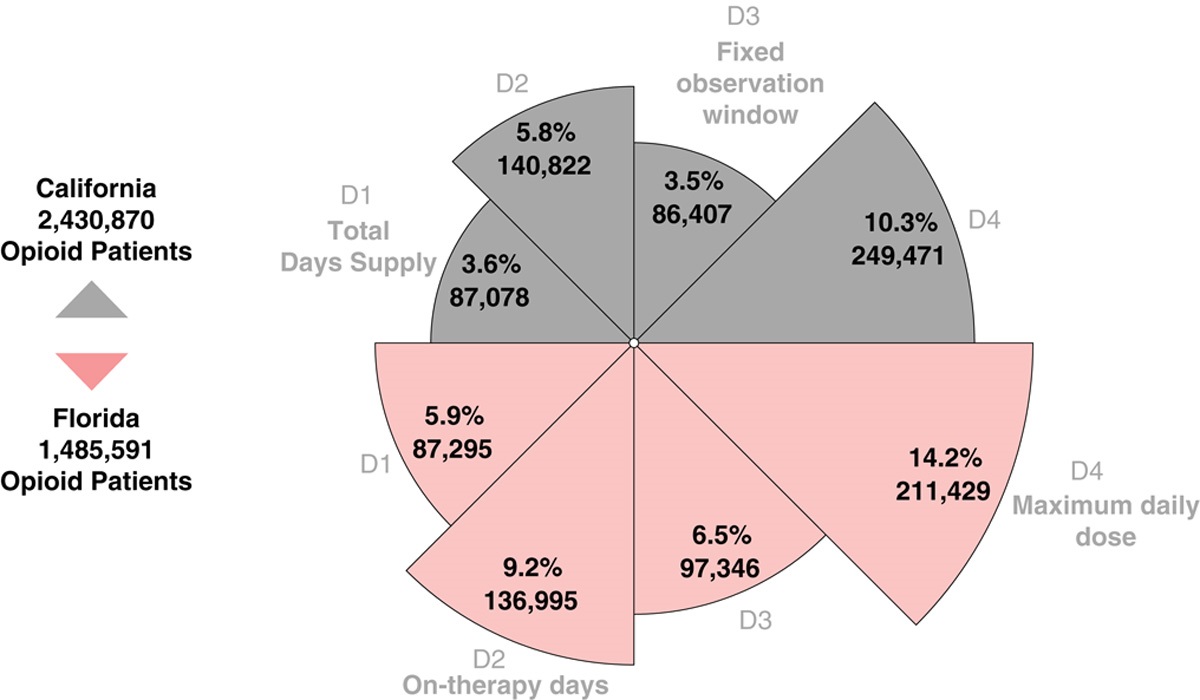
nition” of daily MME lacks a clearly defined denominator. Our objective was to assess denominator-dependency on “high dose” classification across competing definitions. Methods: To identify definitional variants, we reviewed literature and electronic prescribing tools, yielding 4 unique...
 journals.lww.com
journals.lww.com
"The overlooked inconsistency among daily MME definitions revealed by our study calls into question the clinical validity of a single numerical risk threshold. When measuring with inches, centimeters, and yards, the absolute number of units is arbitrary. The mix of clinical and research metrics used to calculate the 90 MME threshold is similarly convoluted. As providers, we struggle to do what we feel is right for our patients in the midst of increasing outside pressure with serious ramifications. Our findings call into question state laws and third-party payer MME threshold mandates. Without harmonization, the scientific basis for these mandates may need to be revisited. As the CDC Guideline is revised, and clinical decision tools are developed, it is critically important to reassess the evidence base in light of this previously unknown MME definitional variability."
Equations for Calculating MMEs | Opioid Research
 www.opioiddata.org
www.opioiddata.org
Last edited: