Makes sense, it's good someone did a study like this. However, even the authors indicate that race should be removed from the equation, but scientists just first need to identify which biological/environmental factors (for which race is currently serving as some sort of proxy) need to be added to the equation to ensure the equation is still accurate.I am aware of that news release. And there has been backlash.
Estimation of Glomerular Filtration Rate With vs Without Including Patient Race
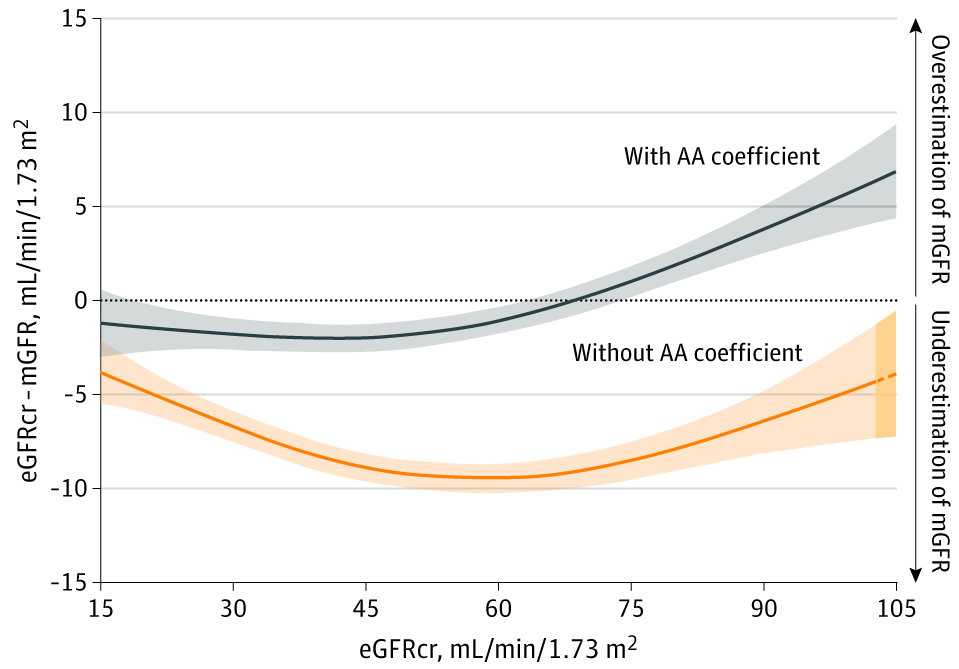
This cross-sectional study evaluates the use of race in estimating glomerular filtration rate and whether height and weight could substitute for race using pooled data from 10 studies of people with and without chronic kidney disease.jamanetwork.com
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Opinion on change.org petition
- Thread starter physiogirl2019
- Start date
-
- Tags
- aamc implicit bias nbme petition race

- Joined
- Jun 17, 2015
- Messages
- 3,043
- Reaction score
- 4,029
- Points
- 7,041
- Medical Student
Makes sense, it's good someone did a study like this. However, even the authors indicate that race should be removed from the equation, but scientists just first need to identify which biological/environmental factors (for which race is currently serving as some sort of proxy) need to be added to the equation to ensure the equation is still accurate.
Then would it now follow that the biological factor should be identified before removing the use of the gfr formula.
Yes, that is what I meant when I said that we "first need to identify which biological/environmental factors...need to be added to the equation to ensure the equation is still accurate." Sorry if I was unclear!Then would it now follow that the biological factor should be identified before removing the use of the gfr formula.
EDIT: I still think it would be good in the meantime to reframe the way it is taught to make sure that students understand this is not due to any inherent difference/inferiority in people of a certain race, but due to other factors that are correlated with belonging to a given social group (often due to things like racism), and that we need more research to be conducted on these factors in order to understand and implement a better GFR formula.
D
deleted480308
Please explain how racism changes gfrYes, that is what I meant when I said that we "first need to identify which biological/environmental factors...need to be added to the equation to ensure the equation is still accurate." Sorry if I was unclear!
EDIT: I still think it would be good in the meantime to reframe the way it is taught to make sure that students understand this is not due to any inherent difference/inferiority in people of a certain race, but due to other factors that are correlated with belonging to a given social group (often due to things like racism), and that we need more research to be conducted on these factors in order to understand and implement a better GFR formula.
Here's a good article explaining the effects of stress on the kidneys and GFR.Please explain how racism changes gfr
Stress and the Kidney - PMC
The prevalence of CKD has increased considerably over the past 2 decades. The rising rates of CKD have been attributed to known comorbidities such as diabetes, hypertension, and obesity; however, recent research has begun to explore the degree to ...
 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
And another if you're interested: Perceived Discrimination and Longitudinal Change in Kidney Function Among Urban Adults - PubMedHere's a good article explaining the effects of stress on the kidneys and GFR.
Stress and the Kidney - PMC
The prevalence of CKD has increased considerably over the past 2 decades. The rising rates of CKD have been attributed to known comorbidities such as diabetes, hypertension, and obesity; however, recent research has begun to explore the degree to ...
D
deleted480308
Did you read that and actually look at the charting, it doesn’t seem to actually show what you seem to be saying it doesAnd another if you're interested: Perceived Discrimination and Longitudinal Change in Kidney Function Among Urban Adults - PubMed
Yes, and I agree with you that in that article the effects are not strong, but the results do indicate an association that mediated by psychosocial (which can also be an affect of racism) and lifestyle factors. Although, I do agree that that is not the best article to support my point.Did you read that and actually look at the charting, it doesn’t seem to actually show what you seem to be saying it does
I guess a better way of explaining the issue with it (as I read more about it as well) is that the current equation is designed with race as a predictor, so it makes sense that removing it will give it worse performance. Instead, it makes more sense to come up with a new equation for measure kidney function that is more precise/accurate for everyone and does not rely on these shortcuts (you can see that the current CKD-EPI equation can be very noisy): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2763564/pdf/nihms132246.pdf (Figure 1)
These were a couple other write-ups that I found helpful in understanding why it is problematic:
Thanks for debating, it helps me understand the issue better as well.
peachrings
Full Member
- Joined
- Apr 16, 2020
- Messages
- 94
- Reaction score
- 162
- Points
- 0
- Medical Student
Yes, and I agree with you that in that article the effects are not strong, but the results do indicate an association that mediated by psychosocial (which can also be an affect of racism) and lifestyle factors. Although, I do agree that that is not the best article to support my point.
I guess a better way of explaining the issue with it (as I read more about it as well) is that the current equation is designed with race as a predictor, so it makes sense that removing it will give it worse performance. Instead, it makes more sense to come up with a new equation for measure kidney function that is more precise/accurate for everyone and does not rely on these shortcuts (you can see that the current CKD-EPI equation can be very noisy): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2763564/pdf/nihms132246.pdf (Figure 1)
These were a couple other write-ups that I found helpful in understanding why it is problematic:
Thanks for debating, it helps me understand the issue better as well.
So its clear, the current equation using race should be used because it is the most accurate currently. Race should not be omitted as a political statement, as UWSOM did. If and when someone comes up with a better equation, we will use that one. This is getting ridiculous.
D
deleted480308
Yes, and I agree with you that in that article the effects are not strong, but the results do indicate an association that mediated by psychosocial (which can also be an affect of racism) and lifestyle factors. Although, I do agree that that is not the best article to support my point.
I guess a better way of explaining the issue with it (as I read more about it as well) is that the current equation is designed with race as a predictor, so it makes sense that removing it will give it worse performance. Instead, it makes more sense to come up with a new equation for measure kidney function that is more precise/accurate for everyone and does not rely on these shortcuts (you can see that the current CKD-EPI equation can be very noisy): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2763564/pdf/nihms132246.pdf (Figure 1)
These were a couple other write-ups that I found helpful in understanding why it is problematic:
Thanks for debating, it helps me understand the issue better as well.
Except the results don’t actually indicate that.
you don’t change an equation until you have a better one, by all means, I’m totally down for a better equation for literally anything
So its clear, the current equation using race should be used because it is the most accurate currently. Race should not be omitted as a political statement, as UWSOM did. If and when someone comes up with a better equation, we will use that one. This is getting ridiculous.
Except the results don’t actually indicate that.
you don’t change an equation until you have a better one, by all means, I’m totally down for a better equation for literally anything
I can't imagine UWSOM would just change the equation solely "as a political statement". It says in their press release that "CKD-EPI results are based on serum creatinine, age, and sex and is normalized to 1.73 m² body surface area" and I don't think they just came up with that out of nowhere and decided to change it without validating it performed at least as well as the old equation. They started looking into this two years ago.
I can't read the full version of the JAMA article you linked before because the full text isn't available, but it doesn't sound from the abstract like they did in that article what UWSOM did. It sounds like they removed the race correction factor altogether and said it performs worse without it (which is in absolutely no way surprising).
I agree that a new, better equation is the best approach and it sounds like in a sense that is what UWSOM did—they developed a modified equation based on the CKD-EPI equation that excluded race and provided similar performance.
D
deleted480308
When you read the uwsom student news releases and here them talking about this as a victory for stopping the teaching the “black bodies are inferior “ you absolutely get to question the impartiality of their opinions. This is activism and not cold/calculating medicine. I’m always ready for a better equation, I just don’t like lies about why the old one is bad.I can't imagine UWSOM would just change the equation solely "as a political statement". It says in their press release that "CKD-EPI results are based on serum creatinine, age, and sex and is normalized to 1.73 m² body surface area" and I don't think they just came up with that out of nowhere and decided to change it without validating it performed at least as well as the old equation. They started looking into this two years ago.
I can't read the full version of the JAMA article you linked before because the full text isn't available, but it doesn't sound from the abstract like they did in that article what UWSOM did. It sounds like they removed the race correction factor altogether and said it performs worse without it (which is in absolutely no way surprising).
I agree that a new, better equation is the best approach and it sounds like in a sense that is what UWSOM did—they developed a modified equation based on the CKD-EPI equation that excluded race and provided similar performance.
A reasonable breakdown of some pros/cons of gfr equations is linked below (free)

Con: Should we abandon the use of the MDRD equation in favour of the CKD-EPI equation?
The best overall index of renal function is the glomerular filtration rate (GFR) [1]. Since measuring the GFR can be cumbersome and costly, estimation of G
 academic.oup.com
academic.oup.com
Unfortunately, no medicine or research is truly impartial as it all reflects the underlying biases of those practicing it. So, of course the folks from UWSOM aren't impartial, but please don't pretend those on the other side of the debate are.When you read the uwsom student news releases and here them talking about this as a victory for stopping the teaching the “black bodies are inferior “ you absolutely get to question the impartiality of their opinions. This is activism and not cold/calculating medicine. I’m always ready for a better equation, I just don’t like lies about why the old one is bad.
A reasonable breakdown of some pros/cons of gfr equations is linked below (free)
Con: Should we abandon the use of the MDRD equation in favour of the CKD-EPI equation?
The best overall index of renal function is the glomerular filtration rate (GFR) [1]. Since measuring the GFR can be cumbersome and costly, estimation of G
- Joined
- Jul 28, 2004
- Messages
- 29,071
- Reaction score
- 63,638
- Points
- 12,236
- Attending Physician
What biases are there in the "don't throw out a decent calculation without having a ready, at least equally good replacement" camp?Unfortunately, no medicine or research is truly impartial as it all reflects the underlying biases of those practicing it. So, of course the folks from UWSOM aren't impartial, but please don't pretend those on the other side of the debate are.
They seem to assume an equation without race is inferior and that race is a robust metric to use to estimate GFR. Do you think the UW group went through two years of development, found the equation didn't work as well, and decided to implement it anyway? I think it is reasonable to assume that a reputable academic institution was responsible enough to perform thorough validation of their new equation before deciding to apply it in clinical practice.What biases are there in the "don't throw out a decent calculation without having a ready, at least equally good replacement" camp?
D
deleted480308
Then show us the study that it’s clearly betterThey seem to assume an equation without race is inferior and that race is a robust metric to use to estimate GFR. Do you think the UW group went through two years of development, found the equation didn't work as well, and decided to implement it anyway? I think it is reasonable to assume that a reputable academic institution was responsible enough to perform thorough validation of their new equation before deciding to apply it in clinical practice.
that’s all I’m asking. You do that, I’ll personally go my own head of nephrology and start the conversation with them. Until then someone talking about “inferiority of black bodies” doesn’t deserve benefit of The doubt
peachrings
Full Member
- Joined
- Apr 16, 2020
- Messages
- 94
- Reaction score
- 162
- Points
- 0
- Medical Student
I can't imagine UWSOM would just change the equation solely "as a political statement". It says in their press release that "CKD-EPI results are based on serum creatinine, age, and sex and is normalized to 1.73 m² body surface area" and I don't think they just came up with that out of nowhere and decided to change it without validating it performed at least as well as the old equation. They started looking into this two years ago.
I can't read the full version of the JAMA article you linked before because the full text isn't available, but it doesn't sound from the abstract like they did in that article what UWSOM did. It sounds like they removed the race correction factor altogether and said it performs worse without it (which is in absolutely no way surprising).
I agree that a new, better equation is the best approach and it sounds like in a sense that is what UWSOM did—they developed a modified equation based on the CKD-EPI equation that excluded race and provided similar performance.
First, the UWSOM press release mentions no hard data validating their new calculation. If it was non-inferior or improved to the current equation with race, I would have expected a publication somewhere. The JAMA article linked in the release is a Viewpoint article, similarly with no hard data. On the other hand, peer reviewed literature links certain genes and haplotypes more prevalent in those of African ancestry to differential rates of CKD and lower eGFR. That's why all this is ridiculous.
Udler MS, Nadkarni GN, Belbin G, et al. Effect of Genetic African Ancestry on eGFR and Kidney Disease. J Am Soc Nephrol. 2015;26(7):1682-92.
Association of trypanolytic ApoL1 variants with kidney disease in African Americans. Science 329: 841–845, 2010
APOL1 genetic variants in focal segmental glomerulosclerosis and HIV-associated nephropathy. J Am Soc Nephrol 22: 2129–2137, 2011
Missense mutations in the APOL1 gene are highly associated with end stage kidney disease risk previously attributed to the MYH9 gene. Hum Genet 128: 345–350, 2010
- Joined
- Jul 28, 2004
- Messages
- 29,071
- Reaction score
- 63,638
- Points
- 12,236
- Attending Physician
Well first, we absolutely know that the standard GFR calculations underestimate GFR in patients of African descent. There's quite a bit of data about that. Barring genetic testing on every patient, race is a decent surrogate.They seem to assume an equation without race is inferior and that race is a robust metric to use to estimate GFR. Do you think the UW group went through two years of development, found the equation didn't work as well, and decided to implement it anyway? I think it is reasonable to assume that a reputable academic institution was responsible enough to perform thorough validation of their new equation before deciding to apply it in clinical practice.
Second, no you can't assume that's true about UW. Like other posters have mentioned, if it was true they'd have published it. If they do, and it's reproducible, I'd also push to start using it.
Then show us the study that it’s clearly better
that’s all I’m asking. You do that, I’ll personally go my own head of nephrology and start the conversation with them. Until then someone talking about “inferiority of black bodies” doesn’t deserve benefit of The doubt
First, the UWSOM press release mentions no hard data validating their new calculation. If it was non-inferior or improved to the current equation with race, I would have expected a publication somewhere. The JAMA article linked in the release is a Viewpoint article, similarly with no hard data. On the other hand, peer reviewed literature links certain genes and haplotypes more prevalent in those of African ancestry to differential rates of CKD and lower eGFR. That's why all this is ridiculous.
Udler MS, Nadkarni GN, Belbin G, et al. Effect of Genetic African Ancestry on eGFR and Kidney Disease. J Am Soc Nephrol. 2015;26(7):1682-92.
Association of trypanolytic ApoL1 variants with kidney disease in African Americans. Science 329: 841–845, 2010
APOL1 genetic variants in focal segmental glomerulosclerosis and HIV-associated nephropathy. J Am Soc Nephrol 22: 2129–2137, 2011
Missense mutations in the APOL1 gene are highly associated with end stage kidney disease risk previously attributed to the MYH9 gene. Hum Genet 128: 345–350, 2010
Well first, we absolutely know that the standard GFR calculations underestimate GFR in patients of African descent. There's quite a bit of data about that. Barring genetic testing on every patient, race is a decent surrogate.
Second, no you can't assume that's true about UW. Like other posters have mentioned, if it was true they'd have published it. If they do, and it's reproducible, I'd also push to start using it.
First, I agree with all of you that I'd like to see the study too. I'm not part of the group, so I don't know why it hasn't been published. For all we know, it's in peer review right now. We'll just have to hope they publish it soon.
Also @peachrings, you're completely right about genetics/ancestry playing a role in disease. A lot of my colleagues study this in cancer. However, ancestry is not the same as race. As discussed in paragraph 1 of the petition, there is a huge range of genetic variability within races, so I agree switching to a genetics/ancestry based approach for determining risk factors would be great.
D
deleted480308
It would be great.....if.....you can show it’s better. And until you have publishable/shareable/reproducible data, I don’t trust a group that speaks more like acitvists than scientistsFirst, I agree with all of you that I'd like to see the study too. I'm not part of the group, so I don't know why it hasn't been published. For all we know, it's in peer review right now. We'll just have to hope they publish it soon.
Also @peachrings, you're completely right about genetics/ancestry playing a role in disease. A lot of my colleagues study this in cancer. However, ancestry is not the same as race. As discussed in paragraph 1 of the petition, there is a huge range of genetic variability within races, so I agree switching to a genetics/ancestry based approach for determining risk factors would be great.
peachrings
Full Member
- Joined
- Apr 16, 2020
- Messages
- 94
- Reaction score
- 162
- Points
- 0
- Medical Student
It would be great.....if.....you can show it’s better. And until you have publishable/shareable/reproducible data, I don’t trust a group that speaks more like acitvists than scientists
Agreed, though I highly doubt they will show non-inferiority. When virtue signalling bleeds over into medicine, we have really gone too far and are now doing harm.
peachrings
Full Member
- Joined
- Apr 16, 2020
- Messages
- 94
- Reaction score
- 162
- Points
- 0
- Medical Student
First, I agree with all of you that I'd like to see the study too. I'm not part of the group, so I don't know why it hasn't been published. For all we know, it's in peer review right now. We'll just have to hope they publish it soon.
Also @peachrings, you're completely right about genetics/ancestry playing a role in disease. A lot of my colleagues study this in cancer. However, ancestry is not the same as race. As discussed in paragraph 1 of the petition, there is a huge range of genetic variability within races, so I agree switching to a genetics/ancestry based approach for determining risk factors would be great.
Currently, a genetics/ancestry approach is not feasible for most healthcare institutions for all patients. Because race has a high correlation with ethnicity, it is still an invaluable variable to have.
This is exactly the bias I referred to in response to the labeling of the UW group as activists/impartial. This doesn’t sound like healthy scientific skepticism: it sounds like you’ve already decided the outcome before seeing the evidence. There’s already evidence that shows race is an imprecise measure. Why is it so hard to be open to the possibility that there could be a way that is more accurate and more inclusive?Agreed, though I highly doubt they will show non-inferiority. When virtue signalling bleeds over into medicine, we have really gone too far and are now doing harm.
Although personalized genomics is already available in some larger centers, I agree that in other centers there is not adequate infrastructure as of yet. But with projects like All of Us in full swing, it is on the horizon. The cost of exome and targeted genomic sequencing is also incredibly low compared to other health expenditures (<$1K) and there are many private companies that can provide access to these technologies in smaller centers/communities. It really is possible in the near future if we choose to invest in it.
peachrings
Full Member
- Joined
- Apr 16, 2020
- Messages
- 94
- Reaction score
- 162
- Points
- 0
- Medical Student
This is exactly the bias I referred to in response to the labeling of the UW group as activists/impartial. This doesn’t sound like healthy scientific skepticism: it sounds like you’ve already decided the outcome before seeing the evidence. There’s already evidence that shows race is an imprecise measure. Why is it so hard to be open to the possibility that there could be a way that is more accurate and more inclusive?
Although personalized genomics is already available in some larger centers, I agree that in other centers there is not adequate infrastructure as of yet. But with projects like All of Us in full swing, it is on the horizon. The cost of exome and targeted genomic sequencing is also incredibly low compared to other health expenditures (<$1K) and there are many private companies that can provide access to these technologies in smaller centers/communities. It really is possible in the near future if we choose to invest in it.
The UW group are essentially activists, if I'm reading the same press release as everyone else. They didn't believe race should be a precision variable, so they tried to make an equation that didn't use race. Discussions in class drove the change, not large patient cohort data. The burden of proof is on those who claim their method is as good/better than the old method. Nowhere is there hard data comparing their new equation to the current standard, which is how proper medical science is done. And in science, if it's not published, it wasn't done.
I agree that race is imprecise and not a perfect measure, but that does not disprove its usefulness. Many measures we use in medicine are imprecise, but we are still better off using them. And who really equates GFR levels to superiority of any kind except these types of activists?
Mass General/Brigham just also removed race from their GFR calculation and cited this article:
They also linked this as a good resource:

 www.nytimes.com
www.nytimes.com
They also linked this as a good resource:
Many Medical Decision Tools Disadvantage Black Patients (Published 2020)
Doctors look to these digital calculators to make treatment decisions, but they can end up denying black patients access to certain specialists, drugs and transplants.
peachrings
Full Member
- Joined
- Apr 16, 2020
- Messages
- 94
- Reaction score
- 162
- Points
- 0
- Medical Student
Again, another viewpoint article with no real data. Even their citations do not have hard data. Any institution that comes up with a non-inferior equation that does not use race will publish it, because that will be a guaranteed NEJM/Lancet paper. And yet, we have not seen a validated/unvalidated equation that is non-inferior. These institutions are trying to bandwagon on the racial justice movement, which I fear will end up hurting the most vulnerable populations.
I'm going to defer to nephrologists on this, I'm just passing along info. This is the explanation in their email:
- Race is a social, not a biologic construct, and the kidney function race multiplier ignores the substantial genetic diversity within self-identified Black patients.
- Research studies have not provided an acceptable scientific rationale for making clinical decisions based on the social construct of race. Prior studies supporting kidney function race multipliers have relied on “examination of skin color” to classify patients.
- Researchers across Mass General Brigham have demonstrated that use of these race multipliers can lead to important delays in care for Black patients, such as timely evaluation for kidney transplantation.
peachrings
Full Member
- Joined
- Apr 16, 2020
- Messages
- 94
- Reaction score
- 162
- Points
- 0
- Medical Student
Race is a social construct but it has a strong correlation with ethnicity which is why empirically, it has worked. Genetic diversity doesn't mean anything because they are looking at all loci, many of which are of unknown significance. If you look at genetic diversity for race and ethnicity within loci of interest (kidney function), the diversity will be much less. Of course, those patients with mixed heritage will be harder to classify accurately. I 100% believe that we should be creating better algorithms accounting for ethnicity and genetic differences. However, until we find one, we should be using the current one, which as it happens takes race into account. We should be relying on empiricism, not philosophy in clinical medicine.
Researchers have also asserted within the same papers (JAMA) that not using the multipliers may lead to inaccurate antibiotic dosing and unnecessary anxiety. These very researchers assert that more research is needed, which is 100% the truth, instead of making decisions by belief, without data, and hoping the empiric data will support those decisions.
Researchers have also asserted within the same papers (JAMA) that not using the multipliers may lead to inaccurate antibiotic dosing and unnecessary anxiety. These very researchers assert that more research is needed, which is 100% the truth, instead of making decisions by belief, without data, and hoping the empiric data will support those decisions.
Similar threads
- Replies
- 2
- Views
- 712
- Replies
- 1
- Views
- 1K