There's a study to show everything, but I don't believe this allegedly-existent one.
Anyone whose ever done more than five spinals for labor knows they are profoundly better than epidurals for the first hour or so ... to the point that one reason some people don't like CSEs, is because they don't like getting called 90 minutes later when the patient perceives that the (normal, functioning, well placed) epidural isn't working right. Because the low dose local + opiate intrathecal dose is that good.
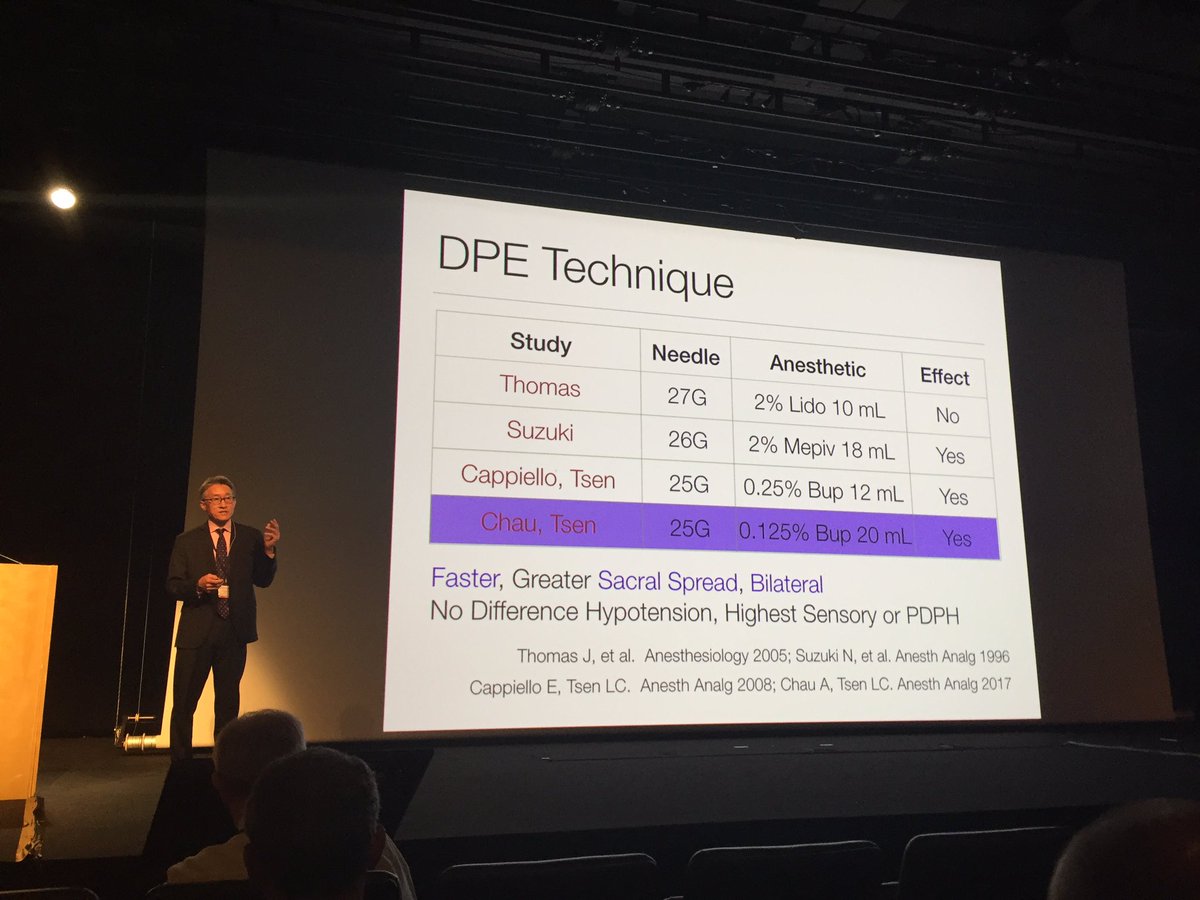
Also, epidurals that are accompanied by a dural puncture (whether a CSE or just a DPE) are possibly superior to straight epidurals, in terms of absolute pain scale and less sacral sparing. I have some issues with the DPE study done at B&W showing how awesome they are, but there's probably some truth to it.
In any case, the CSE is unquestionably better for the first 10-15 minutes. We're not doing them because they're "roughly equivalent" to straight epidurals after 15 or 30 minutes.
Patients love them. They're faster (thread catheter, skip test dose, hit start on pump, leave). I won't be so bold as to claim they're safer (no data to prove it), but I think a procedure that involves bolusing 10+ mL, either via Tuohy or catheter, carries inherently more risk than one that involves bolusing a fraction of a mL followed by starting a slow infusion.

")