You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Propofol shortage
Started by ethilo

D
deleted875186
Biggest challenge would be for MAC. Its easy to do mild to moderate sedation with other drugs, but I don’t know what I would do for deep sedation, which is what most of the surgeons want unfortunately.
There was a propofol shortage in 2011. We used Brevital.
Advertisement - Members don't see this ad
D
deleted875186
There was a propofol shortage in 2011. We used Brevital.
Induction for GA is easy, yoj could use whatever agent you want. Would you use brevital for sedation?
Brevital is longer acting. I suppose it would work for sedation, but you would just have to do intermittent boluses?
Intermittent boluses.
The real alternative if it can’t be done under block and moderate sedation is to just put LMAs in every patient and use Sevo for induction as well.
The real alternative if it can’t be done under block and moderate sedation is to just put LMAs in every patient and use Sevo for induction as well.
Midazolam
I heard people were doing endo with etomidate during the last shortage. Sounds barbaric.
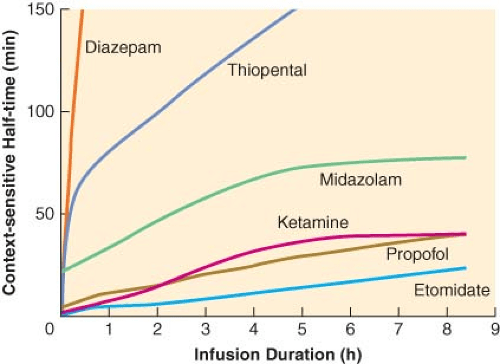
Etomidate is actually a great sedation drug. It's titratable and has the most favorable context-sensitive half time out of any drug out there.I heard people were doing endo with etomidate during the last shortage. Sounds barbaric.
I heard people were doing endo with etomidate during the last shortage. Sounds barbaric.
It is also hurts like the dickens on injection and causes a ton of nausea. Not an ideal profile for an ambulatory anesthetic.Etomidate is actually a great sedation drug. It's titratable and has the most favorable context-sensitive half time out of any drug out there.
Advertisement - Members don't see this ad
5000 mOsm is going to do that!It is also hurts like the dickens on injection and causes a ton of nausea. Not an ideal profile for an ambulatory anesthetic.
Mask cases with sevo
There was a propofol shortage in 2011. We used Brevital.
Oh, that was a wonderful ICU month of residency. Everyone on Precedex.
Glad it’s a memory, but shortages are so common of various drugs it keeps you on your toes.
Brevital would be a terrible drug for sedation. It causes a lot of myoclonic movement. It's much, much worse than etomidate. It's so bad that if you use it as an induction drug for general anesthesia with the plan to use a LMA, you'll probably want or need to use muscle relaxant because of the nonstop twitching and hiccuping.Brevital is longer acting. I suppose it would work for sedation, but you would just have to do intermittent boluses?
You'd never get through an endoscopy with it.
I’m surprised nobody mentioned ketamine/versed combo. Would work fine for GA induction, and ketamine works wonders for sedation for burn dressing changes. A 0.5-0.75 mg/kg bolus up front followed by 10-20 mg bolus intermittently seems to produce a pretty zonked patient who tolerates pretty painful/stimulating stuff. Heck it even helps lube the endoscope for the EGD, and encourages spontaneous ventilation
Except there's currently a ketamine shortage as well..
I’m surprised nobody mentioned ketamine/versed combo. Would work fine for GA induction, and ketamine works wonders for sedation for burn dressing changes. A 0.5-0.75 mg/kg bolus up front followed by 10-20 mg bolus intermittently seems to produce a pretty zonked patient who tolerates pretty painful/stimulating stuff. Heck it even helps lube the endoscope for the EGD, and encourages spontaneous ventilation
Except there's currently a ketamine shortage as well..
Touché
I’m surprised nobody mentioned ketamine/versed combo. Would work fine for GA induction, and ketamine works wonders for sedation for burn dressing changes. A 0.5-0.75 mg/kg bolus up front followed by 10-20 mg bolus intermittently seems to produce a pretty zonked patient who tolerates pretty painful/stimulating stuff. Heck it even helps lube the endoscope for the EGD, and encourages spontaneous ventilation
With the amount of **** coming out of patients' mouths during upper endoscopies/ERCPs even with plain ol' propofol, giving ketamine on top would lead me to worry that they would be have a higher chance of aspirating. Maybe premedicate them with a little glyco if you think it's going to be a longer endoscopy/ERCP?
Definitely does sound like a good drug to be able to fall back on for these procedures if there is a propofol shortage...will have to try it sometime.
They should just shut the hospital down. Do only urgent and emergent cases.
D
deleted162650
They should just shut the hospital down. Do only urgent and emergent cases.
You’re clearly salaried.
Advertisement - Members don't see this ad
You’re clearly salaried.
I was facetious. But I do think it is BS to deal with these drug shortages on a near daily basis. We aren't a 3rd world country
ERCP always intubated at multiple places I've worked.With the amount of **** coming out of patients' mouths during upper endoscopies/ERCPs even with plain ol' propofol, giving ketamine on top would lead me to worry that they would be have a higher chance of aspirating. Maybe premedicate them with a little glyco if you think it's going to be a longer endoscopy/ERCP?
Definitely does sound like a good drug to be able to fall back on for these procedures if there is a propofol shortage...will have to try it sometime.
ERCP always intubated at multiple places I've worked.
institution dependent. we mostly MAC our ERCP's.
ERCP always intubated at multiple places I've worked.
Believe it or not, anesthetics can be performed in different ways! 😱
For real though, in training we did almost every ERCP under MAC. In practice, I do a combination of both, and make my decision based on the GI docs speed, sickness of the patient, etc etc
In my Hospital, I use TSE mask + propofol only for the patients under ERCP procedure. The results are ok!ERCP always intubated at multiple places I've worked.
Oh god I remember the propofol shortage of 2011, it was a nightmare.In the spirit of opioid shortages, what would you do if there was a propofol shortage? I'm curious of people's plans for various anesthetic scenarios.
The last propofol shortage was a factory issue, as most of our meds are manufactured overseas and the factory processing propofol was found to be far less than sterile. It lasted for the better part of a year in my area, and I was working the ICU so you can imagine that we don't have the option of shutting down for a year lolI was facetious. But I do think it is BS to deal with these drug shortages on a near daily basis. We aren't a 3rd world country
D
deleted171991
Look up the threads from 6-8 years ago, and you'll find the answers. 😉In the spirit of opioid shortages, what would you do if there was a propofol shortage? I'm curious of people's plans for various anesthetic scenarios.
D
deleted171991
Greeeedy! I mean... Saaaalty!You’re clearly salaried.
D
deleted171991
BREVItal is longer acting than what?Induction for GA is easy, yoj could use whatever agent you want. Would you use brevital for sedation?
Brevital is longer acting. I suppose it would work for sedation, but you would just have to do intermittent boluses?
Advertisement - Members don't see this ad
D
deleted171991
+1. Or etomidate. Or ketamine.There was a propofol shortage in 2011. We used Brevital.
Of course ERCP can be done under MAC. Then again, when you look at all the secretions on the patients pillow at the end of it and realize you're actually giving GA without the ability of the patient to protect their airway, why do you think it's a good idea to do it under MAC?
I've seen someone do a one level laminectomy under MAC. It can be done, Doesn't make it smart. Anesthesia is all about limiting risk, not about getting away with it.
I've seen someone do a one level laminectomy under MAC. It can be done, Doesn't make it smart. Anesthesia is all about limiting risk, not about getting away with it.
Haldol + Versed + Titrated Fentanyl is another option for MAC
D
deleted87051
MAC ERCP=waiting for coughing, sputtering, desaturation.
GA/ETT ERCP=Kick back and chillax.
GA/ETT ERCP=Kick back and chillax.
Remifenatnil + midazolam isn’t a bad choice either.Etomidate is actually a great sedation drug. It's titratable and has the most favorable context-sensitive half time out of any drug out there.
I have started to become more leery of etomidate. I’m not sure we don’t hurt people with it.
That had been much of my mindset, especially when I discover that one indication for etomidate was adrenal suppression in patients with Cushing syndrome.Remifenatnil + midazolam isn’t a bad choice either.
I have started to become more leery of etomidate. I’m not sure we don’t hurt people with it.
That said, nothing out there as far as data supports any increase in mortality from the adrenal suppression. Take it FWIW, but a Cochrane review is out there without any increase in mortality related to etomidate use Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients
Granted as an anesthesiologist, there are cleaner ways to put a sick patient to sleep. But I do think its harm is overblown. Especially when compared to ketamine (taking myocardial depression into account) and propofol. You've also got to consider that a lot of cardiac cases are done using etomidate solely and in the hands of a less-experienced provider (ED, ICU) it really shouldn't be as demonized as it is.
That had been much of my mindset, especially when I discover that one indication for etomidate was adrenal suppression in patients with Cushing syndrome.
That said, nothing out there as far as data supports any increase in mortality from the adrenal suppression. Take it FWIW, but a Cochrane review is out there without any increase in mortality related to etomidate use Single induction dose of etomidate versus other induction agents for endotracheal intubation in critically ill patients
Granted as an anesthesiologist, there are cleaner ways to put a sick patient to sleep. But I do think its harm is overblown. Especially when compared to ketamine (taking myocardial depression into account) and propofol. You've also got to consider that a lot of cardiac cases are done using etomidate solely and in the hands of a less-experienced provider (ED, ICU) it really shouldn't be as demonized as it is.
The (admittedly) retrospective paper from 2013 hat showed a large increase in OR for 30 day mortality has me looking for other ways to get people to sleep.
Similar threads
- Replies
- 14
- Views
- 2K