Sanman
O.G.
- Joined
- Sep 2, 2000
- Messages
- 6,722
- Reaction score
- 11,217
No, no, no, didn't you get the memo?CBTchemotherapy is shallow and doesn't consider the whole person! 🙄
Fixed. Curious what they would say about that.

No, no, no, didn't you get the memo?CBTchemotherapy is shallow and doesn't consider the whole person! 🙄
As much as I hear psychodynamic/psychoanalytic folks whine about pro-CBT bias in the field, it’s certainly ironic that I hear much more CBT bashing by them than I ever hear psychodynamic bashing from CBT folks.
WUTAnyone else involved in training programs and seeing applicants who talk a lot about IFS? I'm really surprised to see it in doctoral psych programs!
My thing is...not only is IFS just plainly unfalsifiable (I mean, how are we supposed to study these "parts?"), but even if one isn't bothered by the non-empirical nature of it (I am bothered, for the record, but even if one is not), why would someone want to reinforce feelings of multiplicity? Wouldn't the goal of trauma therapy be to promote feelings of integrated identity and sense of self, rather than further reinforce feelings of instability? I would imagine there could be really unfortunate results if this were used on people with BPD or BPD-like traits. Also, interestingly enough, IFS was the modus operandi of the Castlewood Institute, which most here will know was notorious for accepting patients with severe eating disorders as inpatients, only for many of those same patients to end up diagnosed with DID and full of confabulated memories of early childhood abuse. The institute was sued into oblivion and now either doesn't exist or has been rebranded enough to shed its reputation.IFS makes me think of the Inner Child stuff from the 90s. It is obviously true that we learn and develop and practice patterns of relating based on prior experiences but they take it to a woo woo place. I had one friend who liked to joke that he ever found his little child he would beat the crap out of that little bastard. Basically referring to immature and irresponsible patterns of behavior and thinking that he held onto from childhood. The problem I see with this type of “therapy” is that it reinforces maladaptive patterns. My foundations have always been psychodynamic and I just don’t see the need for a conflict between CBT and Attachment theory or Object Relations. My main objection to CBT is I don’t like homework, but that’s a personal issue, not a criticism of the techniques, that’s for sure.
IFS makes me think of the Inner Child stuff from the 90s. It is obviously true that we learn and develop and practice patterns of relating based on prior experiences but they take it to a woo woo place. I had one friend who liked to joke that he ever found his little child he would beat the crap out of that little bastard. Basically referring to immature and irresponsible patterns of behavior and thinking that he held onto from childhood. The problem I see with this type of “therapy” is that it reinforces maladaptive patterns. My foundations have always been psychodynamic and I just don’t see the need for a conflict between CBT and Attachment theory or Object Relations. My main objection to CBT is I don’t like homework, but that’s a personal issue, not a criticism of the techniques, that’s for sure.
Yup. Bad therapy 101. Fragile patients with an unstable sense of self are very vulnerable to this crap.My thing is...not only is IFS just plainly unfalsifiable (I mean, how are we supposed to study these "parts?"), but even if one isn't bothered by the non-empirical nature of it (I am bothered, for the record, but even if one is not) why would someone want to reinforce feelings of multiplicity? Wouldn't the goal of trauma therapy not be to promote feelings of integrated identity and sense of self, rather than further reinforce feelings of instability? I would imagine there could be really unfortunate results if this were used on people with BPD or BPD-like traits. Also, interestingly enough, IFS was the modus operandi of the Castlewood Institute, which most here will know was notorious for accepting patients with severe eating disorders as inpatients, only for many of those same patients to end up diagnosed with DID and full of confabulated memories of early childhood abuse. The institute was sued into oblivion and now either doesn't exist or has been rebranded enough to shed its reputation.
I definitely agree that one could always study the efficacy of the treatment--even if it were shown to be efficacious, though, I would still personally be uncomfortable with it because I don't like the idea of providing clients with explanatory systems/mechanisms which cannot themselves be demonstrated. That's my primary reason for not being super comfortable with psychodynamics--we know they can work very well for some folks, but being unable to demonstrate the existence of the psychodynamic unconscious and the other assumptions of the model makes me shy away from embracing it. I understand that not everyone has that same hangup, though--I just personally feel most comfortable using explanatory/meaning-making systems which can be demonstrated, even if those demonstrations are not perfect.Yup. Bad therapy 101. Fragile patients with an unstable sense of self are very vulnerable to this crap.
As far as research goes, you can’t really study the parts, but you can study the efficacy of using that conceptualization in treatment. It actually wouldn’t be hard to test. The hard part is finding an actual researcher who wants to compare a treatment like CBT to a treatment that is likely to make some patients worse. We tend to wait until lots and lots of people have been harmed before we come to the conclusion that something like this can be harmful.
Oh wow, you opened up a can of memories I forgot I had. Castlewood is still around, it’s called Alasana now, got bought out by private equity, and is expanding faster than it can provide quality care (along with the rest of the eating disorder treatment landscape, sigh.)Also, interestingly enough, IFS was the modus operandi of the Castlewood Institute, which most here will know was notorious for accepting patients with severe eating disorders as inpatients, only for many of those same patients to end up diagnosed with DID and full of confabulated memories of early childhood abuse. The institute was sued into oblivion and now either doesn't exist or has been rebranded enough to shed its reputation.
Operative word being forgot, and not repressed!Oh wow, you opened up a can of memories I forgot I had. Castlewood is still around, it’s called Alasana now, got bought out by private equity, and is expanding faster than it can provide quality care (along with the rest of the eating disorder treatment landscape, sigh.)
I have seen bad therapy called DBT in the community, but everything I have seen points to fairly extensive research about its efficacy. Some has been conducted independently of the Linehan institute as well. Patients of mine that have had good DBT skills training have tools that they can use. One challenge of implementation is that DBT is not psychotherapy and is not a replacement for psychotherapy. So a patient with significant trauma would still need good old fashioned exposure work from a well trained psychotherapist. DBT includes psychotherapy but doesn’t lay out the explicits of that work other than how to address the overall behavioral strategy of some of the safety concerns and the structure of the therapeutic frame. Of course, since many clinicians struggle with these core fundamentals, this alone can be of much use.People in our field keep making up crap like IFS and DBT (without regard to efficacy) because it makes them money!
There are methodological flaws in the research that supposedly demonstrates efficacy. In order to benefit from this "treatment" at all, people have to continue to go to it at a frequency that is not sustainable. People who "graduate" from DBT often "relapse" in a fairly short time after.
Other than that, I suppose it's fine.
I don’t know about the flaws in the research, but the relapse into maladaptive behaviors is consistent with what I see. Given that the prevailing belief in the field that BPD was untreatable and we should curtail how many we worked with prior to DBT, I have witnessed a dramatic shift in outcome and treatment. Also, I don’t think “relapse“ necessarily means treatment didn’t work. As I tell people, patterns repeat and we are looking for a decrease in frequency, intensity, and duration as opposed to an all or none perspective. That makes more sense with substance use than it does with maladaptive patterns related to intense fears of abandonment. I also think that continued treatment and/or support and a recognition of a more lasting continued vulnerability to stress after an intensive phase of DBT is essential.There are methodological flaws in the research that supposedly demonstrates efficacy. In order to benefit from this "treatment" at all, people have to continue to go to it at a frequency that is not sustainable. People who "graduate" from DBT often "relapse" in a fairly short time after.
Other than that, I suppose it's fine.
Any citations to this effect for us to peruse?

 jamanetwork.com
jamanetwork.com
I am fairly positive that research has shown the exact opposite, in fact. Plenty of studies have demonstrated that improvements from DBT are maintained post tx
So in essence, you think that it partly works but after time it loses its effectiveness? If so, I certainly do not want to offer that "treatment" to people knowing it will fail eventually, and also knowing that people with BPD are often quite dangerous.I don’t know about the flaws in the research, but the relapse into maladaptive behaviors is consistent with what I see. Given that the prevailing belief in the field that BPD was untreatable and we should curtail how many we worked with prior to DBT, I have witnessed a dramatic shift in outcome and treatment. Also, I don’t think “relapse“ necessarily means treatment didn’t work. As I tell people, patterns repeat and we are looking for a decrease in frequency, intensity, and duration as opposed to an all or none perspective. That makes more sense with substance use than it does with maladaptive patterns related to intense fears of abandonment. I also think that continued treatment and/or support and a recognition of a more lasting continued vulnerability to stress after an intensive phase of DBT is essential.
So in essence, you think that it partly works but after time it loses its effectiveness? If so, I certainly do not want to offer that "treatment" to people knowing it will fail eventually, and also knowing that people with BPD are often quite dangerous.
And I'm not so sure what 'loses its effectiveness' means (precisely) in this context.This describes the majority of non-surgical treatments in medicine. Do you think internists are a bad idea?
Omg I got a bunch of downvotes for saying that self harm is ineffective coping
In the therapists subreddit
One of the things I will say frequently is that self harm is easier for me to treat than a substance addiction becuase it doesn’t work as well. Replacing it with a more adaptive and effective method such as learning to recognize and express your emotions in a caring relationship beats self harm pretty easy. Drugs of abuse on the other hand tend to easily “win” that comparison. In short, it is pretty low on the effective coping ladder. As far as whether it is adaptive or maladaptive, that’s a little different question. Im pretty sure that ways of improving mindfulness, emotional regulation, interpersonal effectiveness, and distress tolerance are way more in the adaptive camp than either ways of coping.Omg I got a bunch of downvotes for saying that self harm is ineffective coping
In the therapists subreddit
No. It can alleviate the symptoms and teach skills that are lasting, but it doesn’t mean that the person isn’t vulnerabke to relapse and probably needs ongoing less intensive treatment. Especially to work on the interpersonal effectiveness component of DBT which is the hard part for all of us anyway. Dealing with people. The research doesn’t really address this as much because it is more intangible and harder to measure and longer term, but I still think that someone who at their core has a long-standing chronic pattern of unstable relationships is going to need extra work on that. Marsha Linehan says that is the way she sees it pretty directly. Of course, you can always do that through becoming a zen master the way she did since psychotherapists weren’t willing or able to help her but a long term practice of some sorts is kind of assumed.So in essence, you think that it partly works but after time it loses its effectiveness? If so, I certainly do not want to offer that "treatment" to people knowing it will fail eventually, and also knowing that people with BPD are often quite dangerous.
Nah.. I think we're potentially conflating two different things...one is based on an idiographic perspective (judging the efficacy of specific skills taught), the other on a more normative/average (across a number of subjects) perspective (judging the DBT 'package' in terms of loss of tx effects for the avg pt over time at f/u).Given the typical course of mental health and the state of intervention science, I'm hard pressed to think of cases where "It partly works but after time loses its effectiveness" doesn't apply. Maybe exposure treatments for the rare "truly pure" case of PTSD/phobia, or primary insomnia due to obviously-terrible sleep hygiene?
It certainly applies to all psychological interventions for MDD, GAD, SUDs, EDs and most any other bread & butter diagnoses I can think of. Let's be real, curative therapy is the exception and not the rule.
Am I misunderstanding something?
Omg I got a bunch of downvotes for saying that self harm is ineffective coping
In the therapists subreddit
I agree, but I also note that people with BPD are rarely able to engage in the sort of long-term treatment that might be effective.No. It can alleviate the symptoms and teach skills that are lasting, but it doesn’t mean that the person isn’t vulnerabke to relapse and probably needs ongoing less intensive treatment. Especially to work on the interpersonal effectiveness component of DBT which is the hard part for all of us anyway. Dealing with people. The research doesn’t really address this as much because it is more intangible and harder to measure and longer term, but I still think that someone who at their core has a long-standing chronic pattern of unstable relationships is going to need extra work on that. Marsha Linehan says that is the way she sees it pretty directly. Of course, you can always do that through becoming a zen master the way she did since psychotherapists weren’t willing or able to help her but a long term practice of some sorts is kind of assumed.
No of course not, but then again internists don't usually misrepresent what they are doing.This describes the majority of non-surgical treatments in medicine. Do you think internists are a bad idea?
No of course not, but then again internists don't usually misrepresent what they are doing.
If suddenly a treatment were available that arrested the development of a highly deadly cancer and extended survival by 5 years above other treatments, but still usually ended in progression of disease and death, that treatment would immediately become standard of care in oncology. I’m sorry, but I don’t understand how DBT for BPD is pseudoscientific or being misrepresented simply because the individuals receiving treatment are vulnerable to relapse. DBT inarguably is effective at increasing QOL and reducing symptom severity above and beyond alternative options and as such is reasonably the standard of care.I agree, but I also note that people with BPD are rarely able to engage in the sort of long-term treatment that might be effective.
If suddenly a treatment were available that arrested the development of a highly deadly cancer and extended survival by 5 years above other treatments, but still usually ended in progression of disease and death, that treatment would immediately become standard of care in oncology. I’m sorry, but I don’t understand how DBT for BPD is pseudoscientific or being misrepresented simply because the individuals receiving treatment are vulnerable to relapse. DBT inarguably is effective at increasing QOL and reducing symptom severity above and beyond alternative options and as such is reasonably the standard of care.
You are arguing a false equivalency. DBT research is very flawed - something you would presumably know if you were to read it. It is misrepresented often as a "cure" for BPD which it is not. It may or may not increase QOL for friends and relatives of people with BPD (if they have any left), but it is very doubtful that it improves QOL for people who have BPD. That said, I also note that QOL is not a quantitative measure of anything. It is the "standard of care" only because there is nothing else, and at least it gives foolish therapists something to hang on to. I say "foolish" because only a foolish person attempts to treat BPD given that it is untreatable.If suddenly a treatment were available that arrested the development of a highly deadly cancer and extended survival by 5 years above other treatments, but still usually ended in progression of disease and death, that treatment would immediately become standard of care in oncology. I’m sorry, but I don’t understand how DBT for BPD is pseudoscientific or being misrepresented simply because the individuals receiving treatment are vulnerable to relapse. DBT inarguably is effective at increasing QOL and reducing symptom severity above and beyond alternative options and as such is reasonably the standard of care.
You’ve still yet to answer any request for explanation as to why you find the research flawed. It also seems like you carry a very unhealthy and stigmatizing attitude toward people with BPD, who are demonstrably not untreatable and hopeless…it really just seems like you’re arguing out of misplaced emotions than anything.You are arguing a false equivalency. DBT research is very flawed - something you would presumably know if you were to read it. It is misrepresented often as a "cure" for BPD which it is not. It may or may not increase QOL for friends and relatives of people with BPD (if they have any left), but it is very doubtful that it improves QOL for people who have BPD. That said, I also note that QOL is not a quantitative measure of anything. It is the "standard of care" only because there is nothing else, and at least it gives foolish therapists something to hang on to. I say "foolish" because only a foolish person attempts to treat BPD given that it is untreatable.
At best, DBT is a bandaid, and not a very good one.
Read the research yourself, and keep your amateur eval comments to yourself, "Supreme".You’ve still yet to answer any request for explanation as to why you find the research flawed. It also seems like you carry a very unhealthy and stigmatizing attitude toward people with BPD, who are demonstrably not untreatable and hopeless…it really just seems like you’re arguing out of misplaced emotions than anything.
Translation: "I can't actually explain why I think it's bad research so I'll just keep skirting requests to explain myself and demonstrating my ignorance about a whole clinical population by saying that they're untreatable."Read the research yourself, and keep your amateur eval comments to yourself, "Supreme".
You are arguing a false equivalency. DBT research is very flawed - something you would presumably know if you were to read it. It is misrepresented often as a "cure" for BPD which it is not. It may or may not increase QOL for friends and relatives of people with BPD (if they have any left), but it is very doubtful that it improves QOL for people who have BPD. That said, I also note that QOL is not a quantitative measure of anything. It is the "standard of care" only because there is nothing else, and at least it gives foolish therapists something to hang on to. I say "foolish" because only a foolish person attempts to treat BPD given that it is untreatable.
At best, DBT is a bandaid, and not a very good one.
Is it better to have no bandaid? It seems that you consider the alternative to be that BPD is untreatable, and then what? What do you do with these patients who are showing up? If nothing else, we DO know that DBT reduces hospitalizations and overall healthcare utilization/costs. Is that really worse than saying "welp, this is untreatable"?
I also do not think that DBT is promoted as a cure at all, but I suppose it depends on who you talk to.
You do run into this attitude among medical folks sometimes, because they have learned for the purposes of a multiple choice exam at some point that "BPD = refer for DBT" in the same way "syphillis = treat with penicillin." It can also be a way for some psychiatrists to dismiss folks with BPD, "go to DBT (and get out of my office)". More dissemination of GPM is starting to change this (most folks with BPD probably don't need super-specialized treatment if structured correctly) but it's a thing that happens.
EDIT: Zero shade towards DBT, I totally agree about its utility.
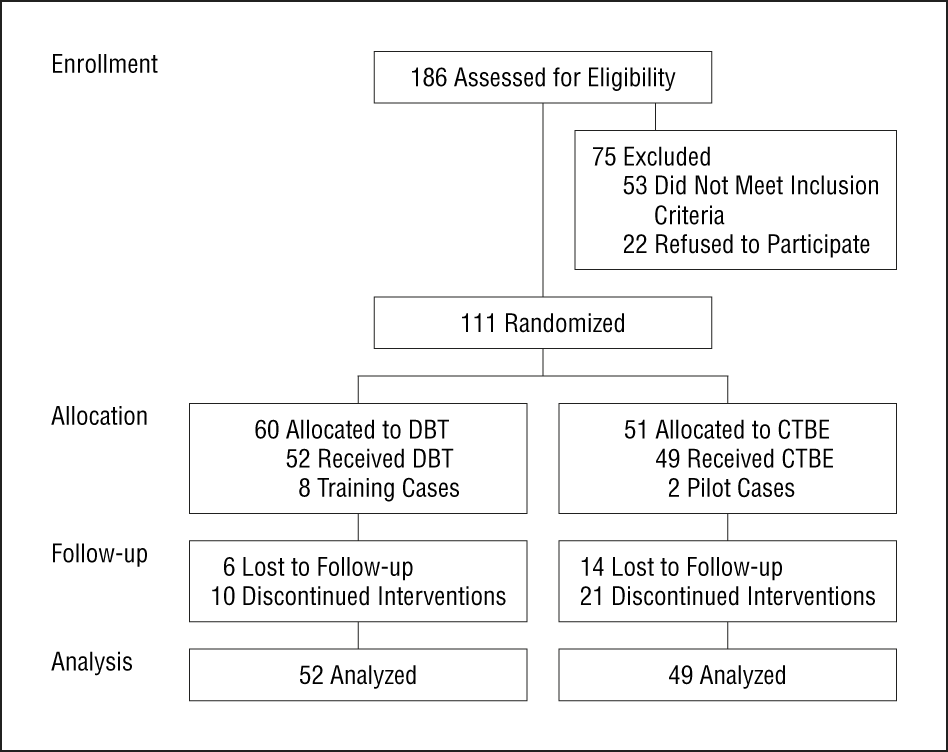
Of course, no bias in this: "Superior performance" blah blah blah. A very representative sample: N = 39 is of course huge, right? Gunderson's Diagnostic Interview for Borderline Personality Disorder was used. No mention of reliability or validity data for this thing at all, and a diagnostic interview was apparently conducted, but no mention of inter-rater relaibility assuming they used more than one interviewer.Like, here's one of the early studies
Naturalistic Follow-up of a Behavioral Treatment for Chronically Parasuicidal Borderline Patients
Background: A randomized clinical trial was conducted to evaluate whether the superior performance of dialectical behavior therapy (DBT), a psychosocial treatment for borderline personality disorder, compared with treatment-as-usual in the community, is maintained during a 1-year...
 jamanetwork.com
jamanetwork.com
This study has multiple serious methodological errors that render the results essentially unreliable.Like, here's one of the early studies
Naturalistic Follow-up of a Behavioral Treatment for Chronically Parasuicidal Borderline Patients
Background: A randomized clinical trial was conducted to evaluate whether the superior performance of dialectical behavior therapy (DBT), a psychosocial treatment for borderline personality disorder, compared with treatment-as-usual in the community, is maintained during a 1-year...
This study has multiple serious methodological errors that render the results essentially unreliable.
This study has multiple serious methodological errors that render the results essentially unreliable.
Perhaps you could link one that you think might possibly be acceptable to real researchers?Perhaps you could point to a psychotherapy RCT that is acceptable to you methodologically?