Thanks for posting your images, that takes guts to do.
First, more likely the patient has developed SIJ pain after the RF than the RF failing. Those SIJs have not moved much for a long time due to pain inhibition. Post RF, the patients move more in the lumbar spine than they have in a long time, which can flare the SIJs. I have to move onto an SIJ injeciton in about approx 5-10% of my lumbar RF patients.
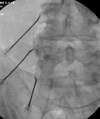
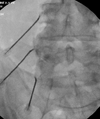
That said, for your needle placement: square the top endplate of L4 and L5, then tilt the II toward the feet 30 degrees, then oblique 20 degrees. For the L5 PDR, square up the top of the sacrum, then tilt II 35 degrees toward the feet, no oblique needed. Then coaxial needle placement to the mamiloaccesory groove.
This will get the active tip more parallel to the nerves. As it appears on these images, the needle tip is at the medial branch but the majority of the acitve tip is lateral to the medial branch.
Also the needles should be placed closer to the neuroforamen.
Your images are better than 99% of people doing this procedure so I mean no offense.