- Joined
- Jul 5, 2016
- Messages
- 245
- Reaction score
- 627
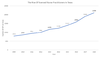
Here in Texas, it seems like almost every nurse I know is taking an online course to be a nurse practitioner. This got me wondering about the numbers of NP's here in Texas.
Looks like numbers have tripled since 2008.
The newest craze in my city seems to be hospitalist who are renting their licenses to these NP's to open up their own family medicine practice and aesthetic practices. There are 4 of them that have opened in the past 2 years in a 10 mile radius of where I live. The doctors appear to almost never be on site since some of these doctors are listed as being in a completely different city who are overseeing the practice. One of them is listed about 400 miles away as having a hosptialist job in another city.
Interestingly, most of the google and yelp reviews are almost all calling their NP---- Dr. John Doe....
I know that competition from midlevels have been a hot topic but it seems that even some our doctor colleagues are willing to sell their license out to midlevels who start up their own practices. Midlevels have a place in medicine but I can't help but get nervous when a brand new graduate from an online NP program opens their own practice, offers botox, weight loss, laser therapies, ADD evaluation and treatment, and typical outpatient primary care treatments.
I have to say that each year I get more and more frustrated by the AMA as our profession is heading towards devaluing our education and profession to this level. All of the midlevels that I've worked with in the past have only had to had 60 hours of in person training per specialty in order go get signed off. That means that thew new online only graduates have only spent 60 hours possibly in primary care before being able to open their own practice after graduation.
Frightening.
I have worked with some brilliant midlevels and in no way mean to bash the whole profession. There can be a well working relationship between physician and midlevel, but I fear we are starting to deviate from what I think that relationship should be. Unsupervised practices with doctors in another city is far from what I imagined.
All data came from Texas Board of Nursing - Nursing Statistics
If you look at the data, the vast majority of midlevels are not going to rural areas but to the main 4 cities in Texas in urban areas.
Looks like numbers have tripled since 2008.
The newest craze in my city seems to be hospitalist who are renting their licenses to these NP's to open up their own family medicine practice and aesthetic practices. There are 4 of them that have opened in the past 2 years in a 10 mile radius of where I live. The doctors appear to almost never be on site since some of these doctors are listed as being in a completely different city who are overseeing the practice. One of them is listed about 400 miles away as having a hosptialist job in another city.
Interestingly, most of the google and yelp reviews are almost all calling their NP---- Dr. John Doe....
I know that competition from midlevels have been a hot topic but it seems that even some our doctor colleagues are willing to sell their license out to midlevels who start up their own practices. Midlevels have a place in medicine but I can't help but get nervous when a brand new graduate from an online NP program opens their own practice, offers botox, weight loss, laser therapies, ADD evaluation and treatment, and typical outpatient primary care treatments.
I have to say that each year I get more and more frustrated by the AMA as our profession is heading towards devaluing our education and profession to this level. All of the midlevels that I've worked with in the past have only had to had 60 hours of in person training per specialty in order go get signed off. That means that thew new online only graduates have only spent 60 hours possibly in primary care before being able to open their own practice after graduation.
Frightening.
I have worked with some brilliant midlevels and in no way mean to bash the whole profession. There can be a well working relationship between physician and midlevel, but I fear we are starting to deviate from what I think that relationship should be. Unsupervised practices with doctors in another city is far from what I imagined.
All data came from Texas Board of Nursing - Nursing Statistics
If you look at the data, the vast majority of midlevels are not going to rural areas but to the main 4 cities in Texas in urban areas.