- Joined
- Feb 17, 2017
- Messages
- 1,521
- Reaction score
- 2,213
to be fair, I'm an M1 and no one here has opened a book beyond FAHadn't opened a book in a year and a half.

to be fair, I'm an M1 and no one here has opened a book beyond FAHadn't opened a book in a year and a half.
to be fair, I'm an M1 and no one here has opened a book beyond FA
I’m not too worried. I’ll stack my training and value, including compensation, as a physician against a NP any day. I think and hope that the public will also recognize the difference.
A colleague of mine had an NP student that is relatively close to graduation following them for a shift. They asked the NP student to list a differential for a patient that they saw together who presented with shortness of breath. The NP student could only think of CHF. When they struggled to think of anything else, my colleague asked them for the differential of any patient with shortness of breath. They still couldn’t say anything else. My colleague then told them, if you don’t think of it, you won’t be able to diagnose it. They asked the NP student to think of more things while they went by themself to see the next patient. I observed the NP student googling shortness of breath. When my colleague returned, again they asked the student to name a differential. The student said, “Well of course CHF, and...” Long pause, then just said, “mitral, like a mitral problem.” They just listed half of a body part. Didn’t even say mitral valve, or a condition like rupture or regurgitation. They couldn’t ever state any of the easy things like AECOPD, asthma exacerbation, pneumothorax, PE, pneumonia, or even CORONER virus when we are in the middle of a pandemic all wearing PPE. Unbelievable.
I also often ask patients who their primary physician is and they sometimes state, “Oh, I just have an NP.” I think patients know the difference.
Compensation shouldn’t ever be equivalent. The competitiveness to get into medical school, knowledge learned, work effort required, and debt undertook should always lead to better compensation. There almost never is a short cut to financial success.
All that being said, there might be a place for NPs. While I appreciate the humor in them grabbing coffee or removing sutures, I do think they can add some value beyond just this. The absolutely have to understand what value they add, their role and the Dunning-Kruger effect. I know what I can’t do as an EP, and they need to recognize what it is they can’t do as non-physicians. If they argue for equivalency to physicians it will lead to their downfall and a wave of litigation.
You mean like the “Rule out PE” that was sent to the ED the other day because the NP pcp had gotten a DDimer for pre-op labs I believe society may tolerate a ‘lower level of care‘ for a perceived, negotiated, cheaper price, but I don’t think they will ever be convinced that the quality is the same. I also don’t think midlevels actually provide cheaper care. Any societal costs of the subsidization of my medical training, or increased costs for my compensation as a physician, are pennies compared to the frequently wrong or unnessary tests/treatment provided by midlevels, even factoring in unnecessary things we do as physicians to decrease medicolegal risk or increase patient satisfaction.
I believe society may tolerate a ‘lower level of care‘ for a perceived, negotiated, cheaper price, but I don’t think they will ever be convinced that the quality is the same. I also don’t think midlevels actually provide cheaper care. Any societal costs of the subsidization of my medical training, or increased costs for my compensation as a physician, are pennies compared to the frequently wrong or unnessary tests/treatment provided by midlevels, even factoring in unnecessary things we do as physicians to decrease medicolegal risk or increase patient satisfaction.
I believe society may tolerate a ‘lower level of care‘ for a perceived, negotiated, cheaper price, but I don’t think they will ever be convinced that the quality is the same. I also don’t think midlevels actually provide cheaper care. Any societal costs of the subsidization of my medical training, or increased costs for my compensation as a physician, are pennies compared to the frequently wrong or unnessary tests/treatment provided by midlevels, even factoring in unnecessary things we do as physicians to decrease medicolegal risk or increase patient satisfaction.
I think MLPs are best utilized when they do what you tell them to do.
White magic is nice and easy.
Science is hard.
Patient sent to me for admission last night by Jenny McJennyson, NP-ABC123.
67 year old female "cellulitis of both legs unresponsive to antibiotics"
This poor woman was given augmentin, bactrim, and doxy with no improvement in her bilateral tib/fib cellulitis for a month. Now Jenny McJennyson sent the patient to me for admission and "IV antibiotics, because they're stronger."
Made the diagnosis in 5 seconds.
Stasis dermatitis with hemosiderin deposition. No cellulitis, whatsoever.
Patient is insistent that she was sent by "Doctor Jenny" for admission and IV antibiotics.
I wanted to punch Dr. Jenny in the mouth.
This was after Mackenzie McNurseasaurus sent me a patient from urgent care for HTN with a pressure of 16X/8X, because that's really high for him and I told him that he doesn't want to have a stroke so he needs to go RIGHT NOW." (SHE ACTUALLY FREAKING SAID THIS!)
Mackenzie actually picked up the phone to call me and let me know of this urgent referral!
I actually had her Google search the guidelines while I was on the phone with her.
Crickets.
I wanted to reach thru the phone and punch Mackenzie in the mouth.
Ahem.
If they do what we say; and we tell them not to fight back, then they won't fight back.
Duh.
There. Now that I got the jokes out of my system.
Good post. I have some stuff to add; will formulate an ordered response in a bit. Just got back from the gym.
This one doesn't work, because the paralegal can't argue cases in court. The mid-level can see pts just like we can (I mean, filling the same space).Same goes for a paralegal and a lawyer.
This one doesn't work, because the paralegal can't argue cases in court. The mid-level can see pts just like we can (I mean, filling the same space).
We could call them APPs. Advance Practice ParalegalsYeah that’s a mistake. They should be more like paralegals.

I can confidently say exactly 0 interns in this country would of made this mistake. The lack of understanding of basic pathophysiology with nps is what strikes me the most.‘The misdiagnosis ended up costing her, her life’: A Texas family’s warning for all parents
“The misdiagnosis ended up costing her, her life,” Betty Wattenbarger’s dad said. “There were a lot of things that were missed.”www.kxan.com
‘The misdiagnosis ended up costing her, her life’: A Texas family’s warning for all parents
“The misdiagnosis ended up costing her, her life,” Betty Wattenbarger’s dad said. “There were a lot of things that were missed.”
NP is the biggest joke. The barrier to entry is unbelievably low. I wouldn't send my dog to an NP.
That's part of the frustrating part - we go through med school, take the MCAt to get in, go through rigorous medical training take steps 1-3 - for what!!!, then get through residency, then as if that's not enough take boards I, then boards II! why!
when NP's are "comparable" yet have 1/3 of the training. then aren't we saying that the rigor and training doctors go through is excessive?!
More like 1/10.
‘The misdiagnosis ended up costing her, her life’: A Texas family’s warning for all parents
“The misdiagnosis ended up costing her, her life,” Betty Wattenbarger’s dad said. “There were a lot of things that were missed.”
‘The misdiagnosis ended up costing her, her life’: A Texas family’s warning for all parents
“The misdiagnosis ended up costing her, her life,” Betty Wattenbarger’s dad said. “There were a lot of things that were missed.”
Jesus, she looks periarrest
Im an ER nurse and even I wouldn't have sent that child home based solely on the picture. I don't think that NP training is the problem, I think that the lack of an experience requirement to get into an NP school is the problem.I was thinking the same thing. It bothered me a lot seeing her picture knowing that someone sent that child home like that (if the caption is correct that the photo was snapped in the waiting room).
I know as a resident if I tried to discharge that kid from a peds rotation, my RNs there would have refused and immediately called the charge nurse to go over my headIm an ER nurse and even I wouldn't have sent that child home based solely on the picture. I don't think that NP training is the problem, I think that the lack of an experience requirement to get into an NP school is the problem.
Imo, any RN with 2-3 years of experience in the ER or ICU would have sent this patient to an ER.
Im an ER nurse and even I wouldn't have sent that child home based solely on the picture. I don't think that NP training is the problem, I think that the lack of an experience requirement to get into an NP school is the problem.
Imo, any RN with 2-3 years of experience in the ER or ICU would have sent this patient to an ER.
If we are comparing their care to that of an MD/DO, then I'd agree. To clarify, I think that NP's with RN experience are adequately trained to treat patients under direct physician supervision. However, my experience with NP's is limited. We have a surgical NP that assists in surgery and rounds on patients post op. She is very good at her job. The NP's that we have in the ED see fast track patients (level 3 trauma center) and their charts are reviewed by a physician prior to dispo. I personally haven't seen much of a difference between our PA's and NP's.NP training (or lack thereof) is most certainly the problem. They write discussion posts talking about feelings, take online exams, and don't read books. Their clinical training is not standardized. They can rotate with any person. It is a JOKE. I've witnessed it first hand.
I advocate whole heartedly for PA > NP. I would gladly see a PA for my own care; NEVER an NP.
No they aren’t adequately trained.If we are comparing their care to that of an MD/DO, then I'd agree. To clarify, I think that NP's with RN experience are adequately trained to treat patients under direct physician supervision. However, my experience with NP's is limited. We have a surgical NP that assists in surgery and rounds on patients post op. She is very good at her job. The NP's that we have in the ED see fast track patients (level 3 trauma center) and their charts are reviewed by a physician prior to dispo. I personally haven't seen much of a difference between our PA's and NP's.
If used properly, I don't believe that training is a huge issue. Just my opinion.
Based on what?No they aren’t adequately trained.
Based on them having no clue what the **** is going on, literally 90% of the time?Based on what?
You'd have to have some way of actually proving this claim.
So you believe that a PA and NP, both practicing under direct physician supervision, wouldn't have similar outcomes due to the PA's superior training?
Do you believe that facilities continue to hire NP's despite having PA's in similar roles that are much more productive?
So no proof at all?Based on them having no clue what the **** is going on, literally 90% of the time?
Based on what?
You'd have to have some way of actually proving this claim.
So you believe that a PA and NP, both practicing under direct physician supervision, wouldn't have similar outcomes due to the PA's superior training?
Do you believe that facilities continue to hire NP's despite having PA's in similar roles that are much more productive?
TNTCSo no proof at all?
Based on what?
You'd have to have some way of actually proving this claim.
So you believe that a PA and NP, both practicing under direct physician supervision, wouldn't have similar outcomes due to the PA's superior training?
Do you believe that facilities continue to hire NP's despite having PA's in similar roles that are much more productive?
So no proof at all?
Based on what?
You'd have to have some way of actually proving this claim.
So you believe that a PA and NP, both practicing under direct physician supervision, wouldn't have similar outcomes due to the PA's superior training?
Do you believe that facilities continue to hire NP's despite having PA's in similar roles that are much more productive?
I didn't ask for physicians to provide any proof. I asked a single individual to provide proof to support his claimThe burden of proof does not lie with physicians to demonstrate that nurse practitioners do not provide what is considered standard medical care, especially if they wish to practice independently.
A ton of assumptions here and complete disrespect for multiple professions. I think that you'd be surprised if you sat in on lectures at some of the top nursing schools. I'm not sure how current medicine would even function without midlevels.You claim one NP "does a good job" and cite that as a source for them being competent playing a provider role. Then you add on mundane requirements such as 3 years RN experience. Unless you are surgeon in that field how do you even know they are providing adequate care? RN experience is nothing like doctor experience, which med students are taught starting day one. Yes it teaches you the workflow of the hospital but that is about it. You never think like a doctor (MD/DO), because you don't have the foundations. Nurse's are taught basic principles and checklist medicine. MD/DOs are taught to follow scientific model and to think independently, challenge everything that doesn't make sense. We have different roles that are equally important for there own reasons. However, no nurse should be in charge patient care without going to medical school first. NPs only exist to keep costs down and allow lazy doctors to work less/make more. PAs shouldn't exist either, but they are taught a similar model to MD/DOs and are taught to ask medical doctors for help when they need it. Nurse are told to document 'MD aware."
What the eyes cant see the mind doesn't know.
A ton of assumptions here and complete disrespect for multiple professions. I think that you'd be surprised if you sat in on lectures at some of the top nursing schools. I'm not sure how current medicine would even function without midlevels.
At some point opinions need to be backed by facts. I've never met an MD/DO that shares your opinions, and people talk a lot in the hospital. I've also never witnessed a huge difference between midlevel providers. Our NP's actually have higher patient satisfaction scores. Only provider I've seen disciplined for lack of productivity was an MD.My medical school had a nursing school with a brick and mortar DNP program. I dated a girl in that program for 2 years and was pretty familiar with their curriculum - I was not impressed with the content covered in nursing school in the slightest.
This was at an ivy-league institution - only God knows what's going down in those online diploma mills.
My subsequent interactions with new NP graduates in the hospital only further reinforced my suspicions that DNP education is full of gaps and insufficient to actually train a provider to do anything beyond the most menial of tasks competently.
As for how medicine would function without midlevels - the United States is the only society that actually employs midlevels to this extent, and by most metrics this system is the most dysfunctional in the western world by a long shot. Literally every society is doing better than us without them, and most people I know find the idea of an independent practitioner with a 2 year degree they got on the internet treating them utterly ghastly.
We never worked in the same systems or talked to the same doctors then...At some point opinions need to be backed by facts. I've never met an MD/DO that shares your opinions, and people talk a lot in the hospital. I've also never witnessed a huge difference between midlevel providers. Our NP's actually have higher patient satisfaction scores. Only provider I've seen disciplined for lack of productivity was an MD.
These horror stories are mostly just online tales
Exactly my point though. If the training was as atrocious as this forum makes it seem, these opinions wouldn't be so rare. This is honestly the only medical forum that I visit with such extreme opinions.We never worked in the same systems or talked to the same doctors then...
At some point opinions need to be backed by facts. I've never met an MD/DO that shares your opinions, and people talk a lot in the hospital. I've also never witnessed a huge difference between midlevel providers. Our NP's actually have higher patient satisfaction scores. Only provider I've seen disciplined for lack of productivity was an MD.
These horror stories are mostly just online tales
 jamanetwork.com
jamanetwork.com
 academic.oup.com
academic.oup.com

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Exactly my point though. If the training was as atrocious as this forum makes it seem, these opinions wouldn't be so rare. This is honestly the only medical forum that I visit with such extreme opinions.
Where are all the patient complaints? Patient deaths? Where is all the data suggesting that PA's have better outcomes?
Where is anything besides anecdotal evidence and opinions that suggest that, in general, nurse practitioners lack the education to properly care for patients?
I dont need data to know that a seatbelt works because it is both common sense and the evidence is everywhere."I think your training pathway sucks and is detrimental to patient care without proper oversight" isn't exactly a collegial water-cooler topic of discussion so obviously people aren't going to chat **** about how egregious midlevel training (mostly NP training) is. The internet mostly gives you unfiltered opinions and while a lot of it is noise, the fact that on literally any forum where physicians congregate these opinions are pretty rampant and openly espoused should tell you something.
As for patient satisfaction scores - they mean pretty much nothing in the grand scheme of things. If I gave all of my patients xanax and z packs I could have tremendous satisfaction scores but it doesn't mean I'm doing right by them and plenty of studies suggest that patient satisfaction is negatively correlated with outcomes.
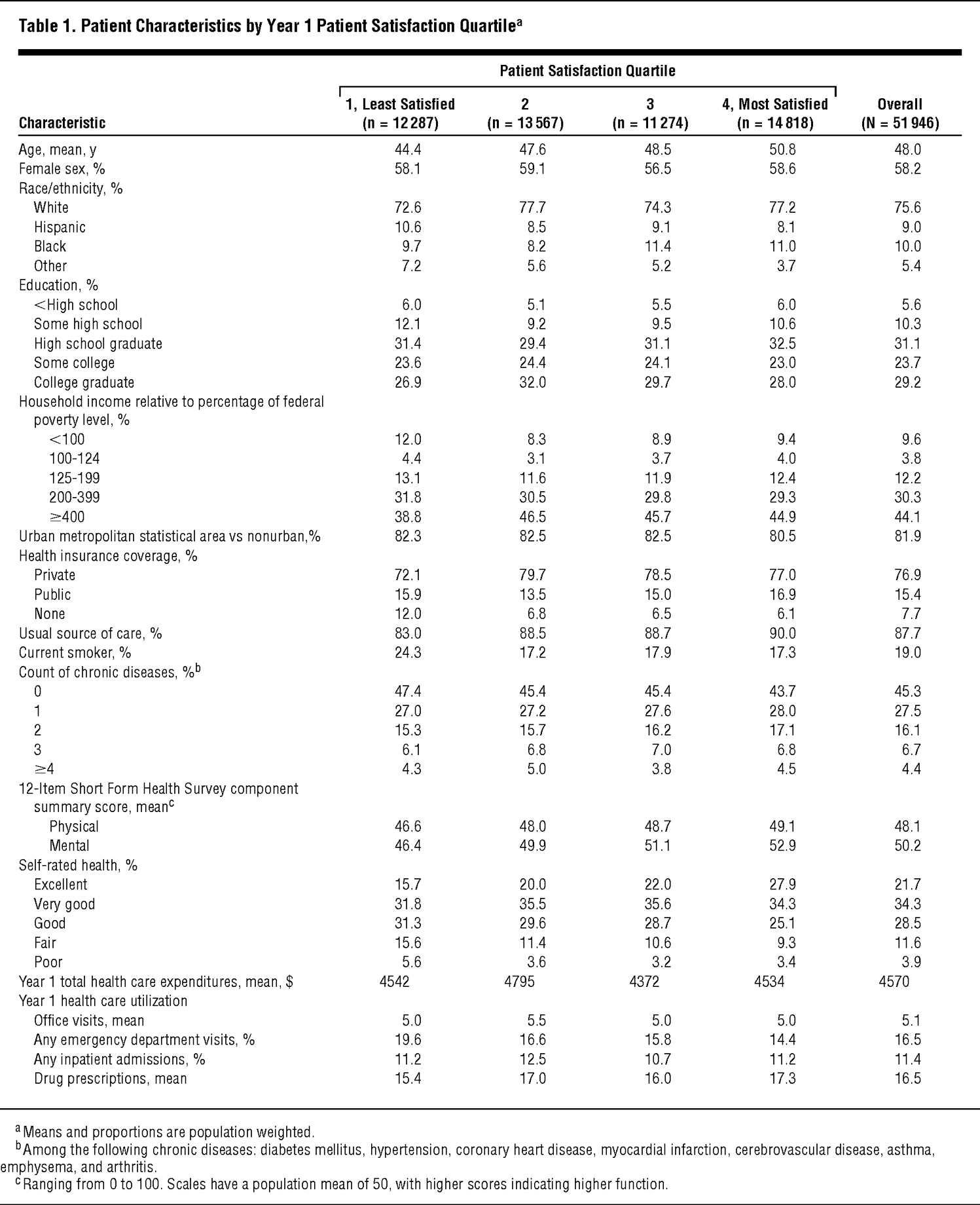
The Cost of Satisfaction
Background Patient satisfaction is a widely used health care quality metric. However, the relationship between patient satisfaction and health care utilization, expenditures, and outcomes remains ill defined.Methods We conducted a prospective cohort study of adult respondents (N = 51 946) to the...
Neurosurgery
The cost of satisfaction: a national study of patient satisfaction, health care utilization, expenditures, and mortality - PubMed
In a nationally representative sample, higher patient satisfaction was associated with less emergency department use but with greater inpatient use, higher overall health care and prescription drug expenditures, and increased mortality.
Do you ask for data every time you put on a seatbelt? Or a helmet? Or a parachute?
I mean I've never seen an RCT for skydiving with a parachute vs without, but I imagine the outcomes in the experimental arm would be quite poor.
There are plenty of reasons why there's a lack of robust data truly comparing MDs to midlevels or NPs to PAs. Very few patients will actually agree to be enrolled in a study where their care has literally no physician oversight and the places where patients are desperate enough to do that generally don't have the resources to actually produce quality research. Furthermore, due to most state, local and hospital laws and bylaws, you rarely have midlevels truly alone, and so more often than not somewhere there is somebody (supervising physician, consulting subspecialist, etc) who gets involved before the dumpster fire engulfs the whole neighbourhood. Finally, many of these patients who have no access to physicians also have little or no access to attorneys, so when they suffer the consequences of poor medical care (whether that be at the hands of a midlevel or a doc) they don't have much recourse to seek restitution.