- Joined
- Aug 23, 2014
- Messages
- 3,274
- Reaction score
- 6,647
It is basically a frozen tundra.Why is the marshfield clinic always looking?

It is basically a frozen tundra.Why is the marshfield clinic always looking?
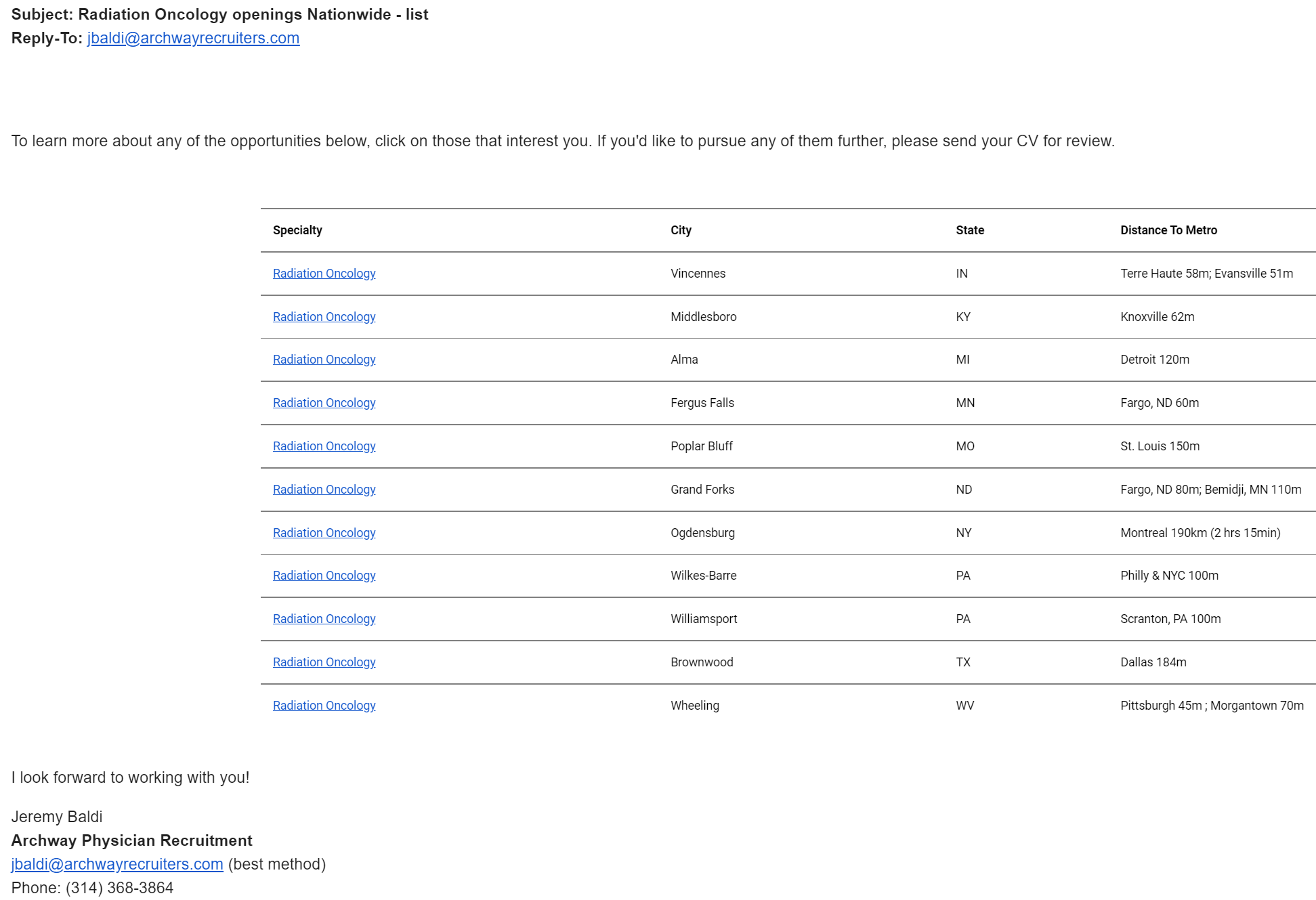
What's BE/BC?Update of the current Astro Career Center Job posting on 6/10/2021:
1) Rad Onc private practice with Lake Region Medical Group (Fergus Falls, MN).
2) Rad Onc private practice with Avera Medical Group (Marshal, MN).
3) Rad Onc private practice with Shorepoint Radiation Oncology Center (Lakewood, NJ).
4) Rac Onc hospital employed at Methodist Hospital (Omaha, NE).
5) Rad Onc academics with Vanderbilt (Nashville, TN).
6) Rad Onc private practice with Herbert Herman Cancer Center (Lansing, MI).
7) Rad Onc academics at Northwell Health at a satellite clinic (Staten Island, NY).
8) Rad Onc private practice with Radiation Oncology Care at Meridian Park (Portland, OR).
9) Rad Onc private practice with and unnamed group (Fredericksburg, VA).
10) Rad Onc private practice with Mercy Clinic (Fort Smith, AR).
11) Rad Onc community academics with U Pittsburg (Williamsport, PA).
12) Rad Onc academics at Henry Ford Health System (Detroit, MI).
13) Rad Onc academic at Yale (New Haven, CT).
14) Rad Onc community academics University of Pennsylvania (Lancaster, PA).
15) Rad Onc private practice with Radiation Oncology Associates of Northern Virginia (Fairfax, VA).
16) Rad Onc hospital employed with Baptist Health Medical Group (New Albany, IN).
17) Rad Onc private practice with Advanced Radiation Centers of NY (Metro NY).
18) Rad Onc community academics at City of Hope (Irvine, CA).
19) Rad Onc private practice with Precision Cancer Care (Kansas City, KS).
20) Rad Onc private practice with Avera Medical Group (Pierre, SD).
21) Rad Onc private practice with Therapy Associates (Evansville, IN).
22) Rad Onc private practice with Spectrum Healthcare Partners (Portland, ME).
23) Derm/Rads part time with Water’s Edge Dermatology (Melbourne, FL).
24) Rad Onc academics with U of Arkansas (Little Rock, AK).
25) Rad Onc hospital employed with Cleveland Clinic (Vero Beach, FL).
26) Rad Onc private practice with US Oncology (Prescott Valley, AZ).
27) Rad Onc hospital employed with Intermountain Healthcare (Logan, UT).
28) Rad Onc hospital employed with Ballad Health (Abingdon, VA).
29) Rad Onc academics LSU/Ochsner (Shreveport, LA).
30) Rad Onc employed at the VA (Memphis, TN).
31) Rad Onc hospital employed at the Marshfield Medical Center (Eau Claire, WI).
32) Rad Onc private practice at Kadlec Clinic (Kennewick, WA).
33) Rad Onc employed at the VA (Jackson, MS).
34) Rad Onc employed at the Guthrie Clinic (Corning, NY).
35) Rad Onc employed at the VA (East Orange, NJ).
36) Rad Onc hospital employed with Geisinger (Danville, PA).
37-bonus) University of Maryland at Baltimore is looking for a PGY-3 resident.
Also saw an ad for New York Urology. 600K guaranteed base with RVU bonus added and 35K sign on bonus. Also tons of heme onc positions listing 500K, 4 days a week, and 100K loan forgiveness. Didn't see a single rad onc job that mentioned salary or bonuses.
Today the Astro website list 361 total MD jobs of which 36 are for BE/BC rad oncs.
What's BE/BC?
 www.wsj.com
www.wsj.com
 www.astro.org
www.astro.org
Aw. They do make it sound wonderful.Astro with the hard sell now
Medical Students - Affiliate - American Society for Radiation Oncology (ASTRO) - American Society for Radiation Oncology (ASTRO)
Are you a medical student who want to learn more about radiation oncology? Learn more about the field, explore FAQ’s on application and interview processes and hear from radiation oncologist about what it’s like to treat and cure cancer patients.
Astro with the hard sell now
Medical Students - Affiliate - American Society for Radiation Oncology (ASTRO) - American Society for Radiation Oncology (ASTRO)
Are you a medical student who want to learn more about radiation oncology? Learn more about the field, explore FAQ’s on application and interview processes and hear from radiation oncologist about what it’s like to treat and cure cancer patients.
Good biryani in those places.oy vey
Fantastic! Even amazing vindalooGood biryani in those places.
I love that for the NY job, the nearest metro is in another country.oy vey
Distance is metric as well.I love that for the NY job, the nearest metro is in another country.
Imagine how the biryani will taste in the places that have jobs in 3-5 years.... Microwaveable, reheated leftoversGood biryani in those places.
You’ll be surprised… Publix actually has some good ones you can reheat. Now do these places have a Publix or even grocery store?Imagine how the biryani will taste in the places that have jobs in 3-5 years.... Microwaveable, reheated leftovers
"Food desert"You’ll be surprised… Publix actually has some good ones you can reheat. Now do these places have a Publix or even grocery store?
Good oxy tooGood biryani in those places.
Kind enough to give the distance in SI units though.I love that for the NY job, the nearest metro is in another country.
Give me Wheeling WV off that list. Live outside washington PA, and you're 30-40 min to work and 30-40 min to Pittsburgh proper.Good biryani in those places.
Oh ya that good WV oxycodone. Some of the best!Good oxy too
To be fair, that’s likely closer than half the UPMC satellites to Pittsburgh.Give me Wheeling WV off that list. Live outside washington PA, and you're 30-40 min to work and 30-40 min to Pittsburgh proper.
Only in the hoity toity neighborhoods, otherwise they are probably better known for methGood oxy too
To each his or her own but unfortunately unlike many other fields, we don’t really have that much of a choice in the matter.I know we like to poke fun, but some of these jobs are not that bad. I'd prefer to have 6-8wk PTO w/4 day work week + make 600k w/ability to travel or FIRE vs. 225k at an academic satellite at UNC.
Who said you get any of that at these places. The trend at the rural places is lower pay, nobody gets 8 weeks I know of... and what is this "4 day work week" of which you speak. Sounds like an Unidentified Aerial Phenomenon.I know we like to poke fun, but some of these jobs are not that bad. I'd prefer to have 6-8wk PTO w/4 day work week + make 600k w/ability to travel or FIRE vs. 225k at an academic satellite at UNC.
Who said you get any of that at these places. The trend at the rural places is lower pay, nobody gets 8 weeks I know of... and what is this "4 day work week" of which you speak. Sounds like an Unidentified Aerial Phenomenon.
You all bring up good points. As a 2022 new grad going through the search...I have realized there is a great deal of variability in jobs. Not just in terms of salary/compensation, but also time off, CME, etc. If you talk to rural docs, many have a pretty good QOL in terms of hours worked, time off, and call responsibilities. The coverage requirements (or lack thereof) have certainly helped. If I end up taking something rural, I will try to negotiate for >700k+ guaranteed. Many places are offering 550k guaranteed for like 2 years + bonus. Some of the job postings state this outright...so no harm in asking for more.
| Vincennes | IN | Terre Haute 58m; Evansville 51m | |
| Middlesboro | KY | Knoxville 62m | |
| Alma | MI | Detroit 120m | |
| Fergus Falls | MN | Fargo, ND 60m | |
| Poplar Bluff | MO | St. Louis 150m | |
| Grand Forks | ND | Fargo, ND 80m; Bemidji, MN 110m | |
| Ogdensburg | NY | Montreal 190km (2 hrs 15min) | |
| Wilkes-Barre | PA | Philly & NYC 100m | |
| Williamsport | PA | Scranton, PA 100m | |
| Brownwood | TX | Dallas 184m | |
| Wheeling | WV | Pittsburgh 45m ; Morgantown 70m |
As a 2022 new grad going through the search...I have realized there is a great deal of variability in jobs.
I locumsed there as resident in early 2000s for 2000day (would never see those rates today through an agency) to buy an engagement ring. remember a patient hitting a deer next to the hospital, and a near brawl starting over how to divide up the carcass with some nearby road workers.I love that for the NY job, the nearest metro is in another country.
Why let the meat go to waste? These are practical folk! I’ll eat any bone thrown my way. This was a preview of the future of our field: take any scraps you can get to survive.I locumsed there as resident in early 2000s for 2000day (would never see those rates today through an agency) to buy an engagement ring. remember a patient hitting a deer next to the hospital, and a near brawl starting over how to divide up the carcass with some nearby road workers.
I locumsed there as resident in early 2000s for 2000day (would never see those rates today through an agency) to buy an engagement ring. remember a patient hitting a deer next to the hospital, and a near brawl starting over how to divide up the carcass with some nearby road workers.
Agree. The numbers people throw around here are completely made up. The range of professional reimbursement 15-20 on treat can give you is so broad I couldn't even quote it here. But to insert some objectivity:@Turaco
I have a lot of familiarity with professional billing and rural positions. It’s my observation that the 15-20 under treat job billing pro fees only won’t get you to $700k unless you have an extraordinary mix of fantastic commercial insurance and tons of Imrt…even then I’m not sure you hit that number.
For that kind of salary I think you’d need to ask for a medical director stipend on top of pro fees…which is completely reasonable in areas hard to recruit.
Could others weigh in here?
I mean you're right. But it may not have to be so out of bounds. Assuming 20 under treatment on average, and averaging 5.5 weeks of treatment per patient, that's 4 new patients a week or 200 new patients a year. At $3500 per patient, you hit $700K. This is how fractionation/treatment style can very dramatically affect private practice salaries though. It's not unreasonable to assume that if your average treatment course per patient is 4 weeks instead of 5.5, you'd average $2500 per patient. And with the same patient load of 4 new patients per week, you're down from $700K collections to $500K collections. After overhead which can easily be 15%, then your salary is doing well if it hits $400-$450K in that rural locale. If you drop from 4 a week to 3 a week because of the latest and greatest not-XRT thing, you're at $300-$350K a year salary.Agree. The numbers people throw around here are completely made up. The range of professional reimbursement 15-20 on treat can give you is so broad I couldn't even quote it here. But to insert some objectivity:
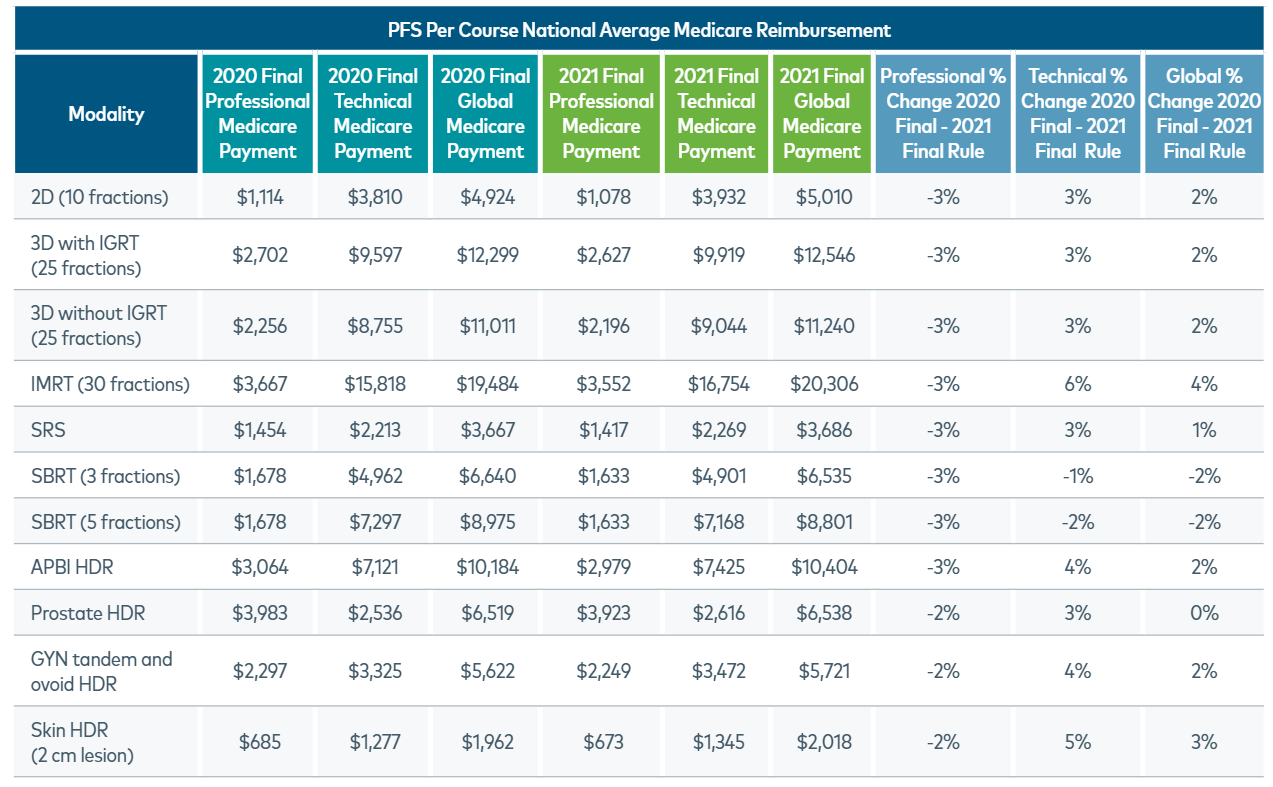
Assume 20 prostates on treatment at all times getting 28 fractions. A reasonable estimate of prof reimbursement at 100% of Medicare is 3,000-ish. The range will probably depend mostly on how you plan (i.e. arcs vs. multi-field IMRT (extra 77300's) and single plan vs. phased plan (additional 77338 and 77300s if you do a boost). (Some insurers are limiting the 77300s, so this may not hold true for long).
52 weeks x 5 days per week= 260 treatment days. (260/28) x 20 x $3,000= $557k. This doesn't take into account holidays, imperfect billing (you'll NEVER collect 100% of what you should be collecting), etc.
So to get to 700k, you would need an average contracted rate of 125% of medicare, 20 IMRT patients on treatment at all times, perfect collections/billing...
Actually I completely agree with your numbers...was gonna post a range of 300k to 700k, but too lazy to go beyond the simplest example. In the absolute worst reimbursing geographies, it could even dip to <250k.I mean you're right. But it may not have to be so out of bounds. Assuming 20 under treatment on average, and averaging 5.5 weeks of treatment per patient, that's 4 new patients a week or 200 new patients a year. At $3500 per patient, you hit $700K. This is how fractionation/treatment style can very dramatically affect private practice salaries though. It's not unreasonable to assume that if your average treatment course per patient is 4 weeks instead of 5.5, you'd average $2500 per patient. And with the same patient load of 4 new patients per week, you're down from $700K collections to $500K collections. After overhead which can easily be 15%, then your salary is doing well if it hits $400-$450K in that rural locale. If you drop from 4 a week to 3 a week because of the latest and greatest not-XRT thing, you're at $300-$350K a year salary.
Then employed positions start looking better.
Yup... Medicare isn't a single payor. Multiple geographic divisions per state in the larger states each with their own reimbursement level, plus many Medicaid/Medicare advantage contracts pay below Medicare rates in more competitive marketsActually I completely agree with your numbers...was gonna post a range of 300k to 700k, but too lazy to go beyond the simplest example. In the absolute worst reimbursing geographies, it could even dip into the 250k range.
Yep, MedMal (>1k per month), DEA/licensing, locums fees for vacations, billing and credentialing (4-10%) may take another 70k+ off your gross collections. The money is in the technical; prof only arrangements aren't always worth the headache especially with the income unpredictability and hassle of finding good coverage.That’s just collections though. Billing will take a cut and there are other costs as mentioned
Good posts above though.
It’s not as simple as just bill your own pro fees…unless a practice has a long history of excellent volumes (regularly 20+).
Things get dicey when when you’re in the 15-20 range.
Would only consider it these days with a generous cut of global collections considering where pro vs technical fees have been going the last several years, as mentioned above. 15 pts isn't a FT pp workload imoThat’s just collections though. Billing will take a cut and there are other costs as mentioned
Good posts above though.
It’s not as simple as just bill your own pro fees…unless a practice has a long history of excellent volumes (regularly 20+).
Things get dicey when when you’re in the 15-20 range.
For the benefit of those looking for jobs now.... This is what admins tell naive physicians in order to manipulate them. Stark law prohibits self-referral by the physician to receive services from entities in which the physician has a financial relationship. As an employed rad onc you aren't making any referrals and you don't own the machines.They may tell you that all employee compensation is reviewed by a consultant so as to not violate Stark Law. The retort to this is, ok I understand that you are worried that you might pay me a salary that my level of work does not justify just so you can recruit somebody way out here. To solve this concern, you can just pay me 100% of my professional collections or allow me to contract with you and do my own billing. That way I am only collecting what I earn and in no way can be in violation of stark law. The hospital will think about this an either reluctantly agree to it or else decide to keep using locums until they find somebody more desperate or less educated (or they will flat out lie and tell you it's still a stark law violation).
I’m in a pro only group. But we’re very busy. I’m happy.
I’d be nervous about pro only (assuming no med director stipend) rural 15 patient set up.
It may be the only option one may have, but I was just posting some thoughts that may be a little divergent from those previously posted.
For the benefit of those looking for jobs now.... This is what admins tell naive physicians in order to manipulate them. Stark law prohibits self-referral by the physician to receive services from entities in which the physician has a financial relationship. As an employed rad onc you aren't making any referrals and you don't own the machines.
They can pay you whatever the hell they want.
Another lie they use is "fair market value," as if they aren't allowed to pay you more than the average rad onc makes in the US.
Bull****... fair market value is whatever it takes to get someone to practice there. 75% MGMA is well within that range.
Which is why I mentioned it depends on geography. It depends on payor mix. Hence my caveat about why it would be a terrible idea in rural Appalachia, but in rural TX where everyone is employed in the beef industry or in the oil fields you could do amazingly well. I had a billing company run numbers for me at a rural practice with about 15-20 on treat and they estimated "conservatively" $900k in pro collections and said it would be very possible to hit 1.2M but did not want to promise me that. Whereas in rural Appalachia, you could be looking at 400k or less as most are medicaid or self-pay.
They took a 5% cut to do the billing, which is fairly typical. Obviously not for everybody, especially new grads who need immediate income coming in. Crucial for hospital employees to understand what the actual collections are when negotiating with the hospital in non-saturated ("take-it-or-leave-it") areas. There is no reason they should not show you data for collections from prior years if you sign an NDA.
Also, it's worth pointing out that the tax loopholes that being self-employed offers you are not insignificant. You can get a large amount of money into tax advantaged accounts with solo 401ks, mega-backdoor roths, etc, as well as writing off business expenses (company car, home office space, etc). Whether that makes more sense for you than a typical hospital benefit package with more affordable health insurance, PTO, and retirement matches is a case-by-case basis. You need a good accountant to advise you.
With a defined benefit cash balance retirement plan, though, isn't your practice on the hook for the value of the investments moving forward? That is, if the market crashes, you have to make up the difference, correct?Yes, good points.
We in our group have opportunity for a defined benefit cash balance retirement plan on top of 401K. A really nice tax avoidance opportunity you don't have as employed (though with caveats it assumes your tax burden in retirement less than what it is now).
With a defined benefit cash balance retirement plan, though, isn't your practice on the hook for the value of the investments moving forward? That is, if the market crashes, you have to make up the difference, correct?
One of the reasons I started posting on sdn was to highlight the obvious that salaries are set by supply and demand. Administrators can certainly pay you in 90% for 30% prodcuctivity, but at some outlying point (95% for 5 %?) it can become a legal issue. Medoncs can get 600k+ easily for 7 k RVUs because that is the market.For the benefit of those looking for jobs now.... This is what admins tell naive physicians in order to manipulate them. Stark law prohibits self-referral by the physician to receive services from entities in which the physician has a financial relationship. As an employed rad onc you aren't making any referrals and you don't own the machines.
They can pay you whatever the hell they want.
Another lie they use is "fair market value," as if they aren't allowed to pay you more than the average rad onc makes in the US.
Bull****... fair market value is whatever it takes to get someone to practice there. 75% MGMA is well within that range.
