- Joined
- Sep 20, 2004
- Messages
- 11,762
- Reaction score
- 11,853
AgreeI am not, but what says it’s isnt
- dose / fractions are sbrt
- volume is small
- Image guided
- breath hold as immobilization
What makes it not sbrt Vs sbrt ?

AgreeI am not, but what says it’s isnt
- dose / fractions are sbrt
- volume is small
- Image guided
- breath hold as immobilization
What makes it not sbrt Vs sbrt ?
Yeah just read it... WildHonestly the initial complaint is not completely terrible but the hearing committee is totally off the rails.
From a cost pov, 5 fx sbrt is equivalent to 15 fx 3d. I'd bet more work goes into apbi from a radonc pov.I am not, but what says it’s isnt
- dose / fractions are sbrt
- volume is small
- Image guided
- breath hold as immobilization
What makes it not sbrt Vs sbrt ?
Chirag wrote this up. It’s more expensive than 3D.From a cost pov, 5 fx sbrt is equivalent to 15 fx 3d. I'd bet more work goes into apbi from a radonc pov.
Sbrt? Could only find report that 5 fx imrt is cheaper than 15 fx 3d.Chirag wrote this up. It’s more expensive than 3D.
Meanwhile on twitter…Tangentially related... academic satellite located into my town a few years back. Over time have shared some bone met patients w/ them. They appear never to have heard of "8 gray in 1 fraction."
Pet scans are so regulated these days... Can't imagine that happening anymore.I heard of someone who has an inhouse PET and owns the machine. They bill globally for this. They get multiple PETs throughout treatment to “guide assessment of response”. Of course many PETs at follow up. This same person treats at 0.5 gy a day treating prostates for months to minimize side effects. Oh and the in house pharmacy brings in lots cheesy dough too.
True story folks!
Personally our field would be better off if FBI would raid all these folks and put them away. Surely they working on it.
The buried lede of this sad story is that multiple radiation oncologists (in what should be the primes of their careers) are available to work whether for Evicore or as physician reviewers for the State Medical Board.Updates....
Former CCS Oncology chief deemed 'danger' to patients, stripped of state medical license
The state Board for Professional Medical Conduct this month revoked the medical license of Dr. Won Sam Yi following a lengthy review of the care he provided to seven seriouslybuffalonews.com
6 weeks of WBRT in a 43 yo F with previous xrt
I don’t think doing an additional CBCT is what makes it SBRT. Many people don’t do multiple images for lung. Your tone is a bit accusatory. What makes this different than other forms of SBRT? It really seems to check the boxes.I am not gonna get sucked into a da worst breast debate but i will briefly answer: the original paper does not call it SBRT. It seems silly to me to go check the CBCT with each treatment, do a second CBCT midway before next arc, and have physics tied up present for treatment when we all know a CBCT with good set up is all that is needed once initial set up is confirmed. This is the kind of stuff that makes us look bad and will continue to put us in crosshair of CMS. I don’t treat breast but in residency when this was done it was never SBRT.
Perhaps but it was for sure going on not too long agoPet scans are so regulated these days... Can't imagine that happening anymore.
I hear ya!I don’t think doing an additional CBCT is what makes it SBRT. Many people don’t do multiple images for lung. Your tone is a bit accusatory. What makes this different than other forms of SBRT? It really seems to check the boxes.
A lot of what you’re saying is institutional policy rather than what defines or is required for SBRT.I am not gonna get sucked into a da worst breast debate but i will briefly answer: the original paper does not call it SBRT. It seems silly to me to go check the CBCT with each treatment, do a second CBCT midway before next arc, and have physics tied up present for treatment when we all know a CBCT with good set up is all that is needed once initial set up is confirmed. This is the kind of stuff that makes us look bad and will continue to put us in crosshair of CMS. I don’t treat breast but in residency when this was done it was never SBRT.
Why are you not billing it if you feel strongly it is sbrt or could be?A lot of what you’re saying is institutional policy rather than what defines or is required for SBRT.
I am not, but what says it’s isnt
- dose / fractions are sbrt
- volume is small
- Image guided
- breath hold as immobilization
What makes it not sbrt Vs sbrt ?
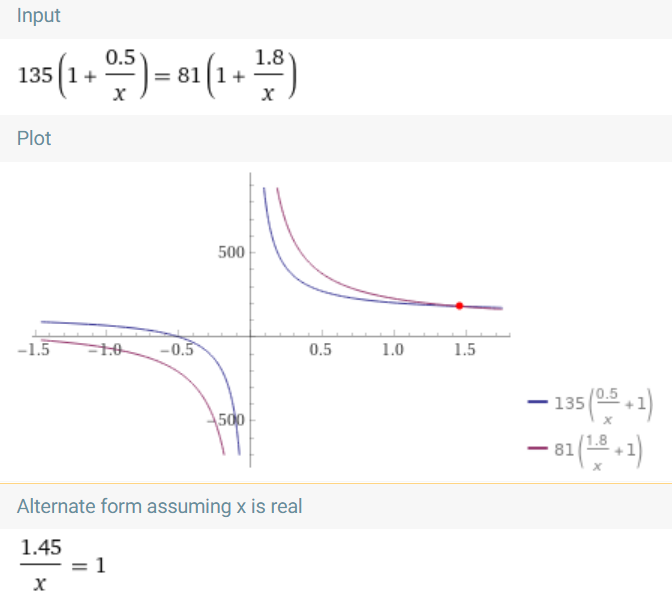
I think it would be >200 fx.Using an alpha beta of 3, 80 fractions of 0.5 gy a day is an EQD2 of 28. You folks do the math
I think there are higher requirements for IGRT QA for SBRT machines, but no reason you couldn’t just use an SBRT-approved machine.I am not, but what says it’s isnt
- dose / fractions are sbrt
- volume is small
- Image guided
- breath hold as immobilization
What makes it not sbrt Vs sbrt ?
It would seem that would be the logical career path. However, if you google him, he appears to be working in Iowa. I guess if you lose your NY license another state will just hand one out.The buried lede of this sad story is that multiple radiation oncologists (in what should be the primes of their careers) are available to work whether for Evicore or as physician reviewers for the State Medical Board.
Chirag wrote this up. It’s more expensive than 3D.
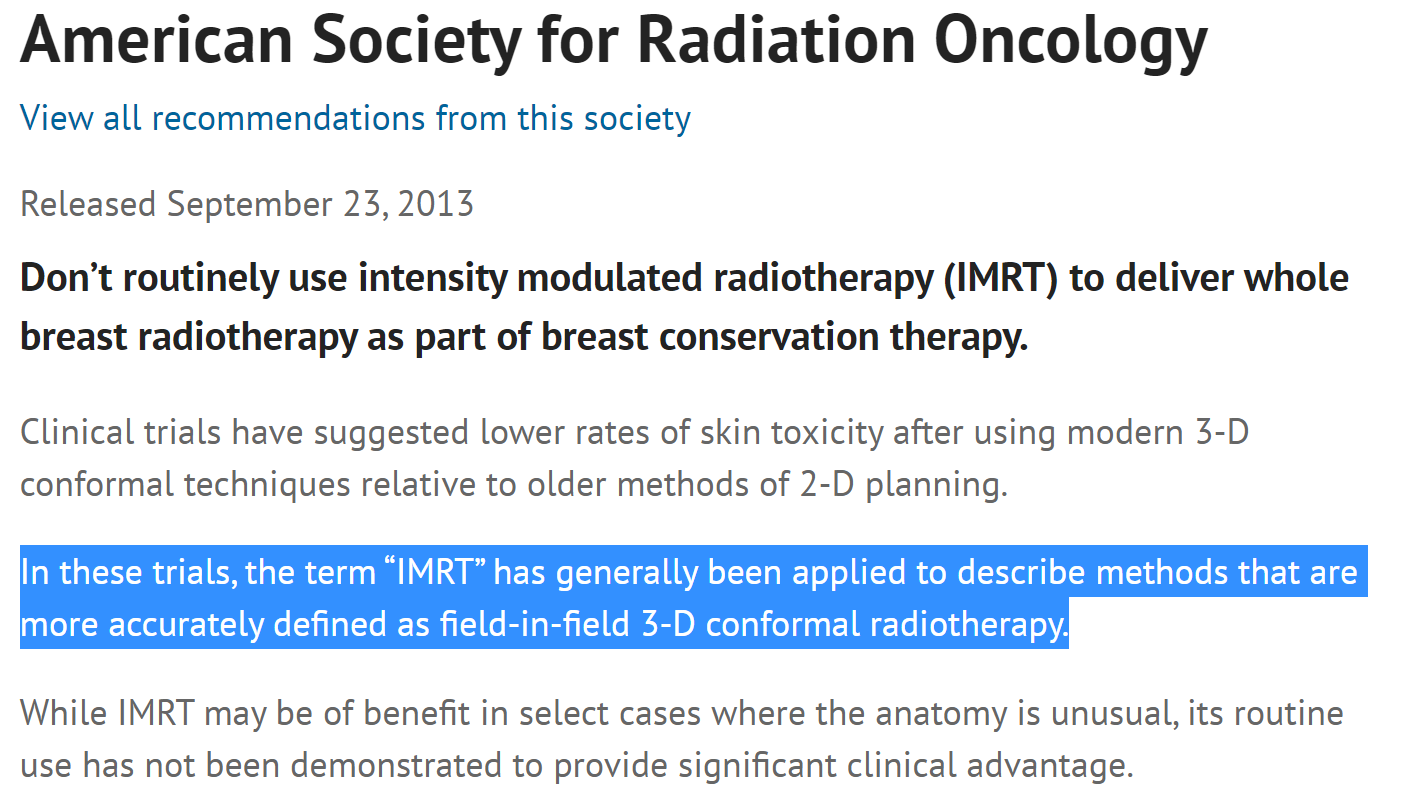
the original paper does not call it SBRT. It seems silly to me to go check the CBCT with each treatment, do a second CBCT midway before next arc, and have physics tied up present for treatment when we all know a CBCT with good set up is all that is needed once initial set up is confirmed.
"[T]he original paper does not call it SBRT."I don’t think doing an additional CBCT is what makes it SBRT. Many people don’t do multiple images for lung. Your tone is a bit accusatory. What makes this different than other forms of SBRT? It really seems to check the boxes.

U gonna type out this beautiful thing yet ignore my request for 0.5 for prostate essay?Sometimes the argument over SBRT vs not SBRT is about feelings, confidence, fear, and subjectivity versus established proscriptive rules, or even science. It's my understanding that 60 Gy in 8 fraction is called, and billed as, SBRT in foreign countries. Foreign countries like Canada. However, in America, if you do 8 fractions of 7.5 Gy per day and try to bill it as SBRT, one of two things will happen:
1) Your stupidity will be exposed and your entire department will hate you because the entire course of therapy will automatically deny upon submission to the payor because, like they say in Maine, "You can't get there from here." Every single payor, including Uncle Sam, in the U.S., has defined SBRT very precisely but broadly...a. Must seek to "eliminate" or "inactivate" a target...b. Must use image guidance, and immobilization...c. Must use 5 fractions or less at >=5 Gy per fraction.That's it.You meet those criteria, it's SBRT.2) You will be put in jail for attempting to commit fraud. (You're still stupid. And American.)But back to feelings and subjectivity. I remember ~20 years ago when the 17 Gy/2 fx lung cancer trial came out in JCO. I mean, for my money, it's one of the slickest pure RT trials in medical history. And I bet 2 (maybe 1?) Americans will have received palliative lung RT of 17 Gy in 2 fractions in 2021. And it's a phIII validated treatment. I think it didn't catch on because... it's frightening! Just like SBRT... very frightening/sphincter tightening (correlates w/ age of rad onc). I got a rad onc guy 20 miles north of me who will never, ever do SBRT (he's about 60yo) because it strikes the fear of God in him. And he has a True Beam. And that 17 Gy in 2 fractions?
I did 17 Gy/2 for obstructing R hilar disease going to hospice… once. Now it is someone else’s turn.Sometimes the argument over SBRT vs not SBRT is about feelings, confidence, fear, and subjectivity versus established proscriptive rules, or even science. It's my understanding that 60 Gy in 8 fraction is called, and billed as, SBRT in foreign countries. Foreign countries like Canada. However, in America, if you do 8 fractions of 7.5 Gy per day and try to bill it as SBRT, one of two things will happen:
1) Your stupidity will be exposed and your entire department will hate you because the entire course of therapy will automatically deny upon submission to the payor because, like they say in Maine, "You can't get there from here." Every single payor, including Uncle Sam, in the U.S., has defined SBRT very precisely but broadly...a. Must seek to "eliminate" or "inactivate" a target...b. Must use image guidance, and immobilization...c. Must use 5 fractions or less at >=5 Gy per fraction.That's it.You meet those criteria, it's SBRT.2) You will be put in jail for attempting to commit fraud. (You're still stupid. And American.)But back to feelings and subjectivity. I remember ~20 years ago when the 17 Gy/2 fx lung cancer trial came out in JCO. I mean, for my money, it's one of the slickest pure RT trials in medical history. And I bet 2 (maybe 1?) Americans will have received palliative lung RT of 17 Gy in 2 fractions in 2021. And it's a phIII validated treatment. I think it didn't catch on because... it's frightening! Just like SBRT... very frightening/sphincter tightening (correlates w/ age of rad onc). I got a rad onc guy 20 miles north of me who will never, ever do SBRT (he's about 60yo) because it strikes the fear of God in him. And he has a True Beam. And that 17 Gy in 2 fractions?
I got it cookin'U gonna type out this beautiful thing yet ignore my request for 0.5 for prostate essay?
Did you bill it as SBRT?!? And are you a Nazi, racist, or both?I did 17 Gy/2 for obstructing R hilar disease going to hospice… once. Now it is someone else’s turn.
I did 17 Gy/2 for obstructing R hilar disease going to hospice… once. Now it is someone else’s turn.
That’s what I said - it’s more expensiveNo.
Dr. shah pub said that 5 fraction IMRT is more cost effective than 15 fraction 3D
SBRT is absolutely more expensive
I’m sure there is a joke there that is just a little too clever for meDid you bill it as SBRT?!? And are you a Nazi, racist, or both?
17/2 is by definition* SBRT by every payor.I’m sure there is a joke there that is just a little too clever for me
got it, thought you were saying 5 fraction imrt was more expensive.That’s what I said - it’s more expensive
What if you make it conformal. Not that conformailty index has anything to do with the proper billing of SBRT, or not.you can make a much better argument that Livi 30/5 is SBRT than 17/2 large field, non-conformal, palliative lung is sbrt. the 17/2 JCO trial was AP/PA.
its not sbrt, by any definition.
what makes 17/2 sbrt more than 8/1?What if you make it conformal.
Some people bill 25/5 for wimpy brain srtwhat makes 17/2 sbrt more than 8/1?
why not bill sbrt for 25/5 rectal?
Now you've got itwhat makes 17/2 sbrt more than 8/1?
why not bill sbrt for 25/5 rectal?
17/2 is by definition* SBRT by every payor.
I would assume you billed it. And I would assume you billed it as SBRT, or not SBRT.
1) If you billed it as SBRT, many people would say you committed fraud.
2) If you didn't bill it as SBRT, CMS could have you for fraudulent under-billing, enticement, etc.
So you're either an over-biller, an under-biller, or both!
* if you used CBCT or kV X-ray or VisionRT for setup
i have no problem with that. its clearly stereotactic technique when youre doing 25/5 for a meningiomaSome people bill 25/5 for wimpy brain srt
i have no problem with that. its clearly stereotactic technique when youre doing 25/5 for a meningioma
Basically we are all saying it is what we say it is.
You're being incredibly subjectivei have no problem with that. its clearly stereotactic technique when youre doing 25/5 for a meningioma
You're being incredibly subjective
What if I do it remotely/non-live, my conformality index is non-incredible, and my Dmax is 107%?live presence, incredible conformality, high heterogeneity
I have tried in the past and failed to get preauth for sbrt 5 gy x 5 rectal. I figured we only get 90% of Medicare from this advantage plan, so why should the hospital not get something reasonable for the treatment.im not arguing there isnt some cognitive dissonance to some of this, but if youre looking at the spectrum of not sbrt to full on SBRT, 25/5 rectal doesnt cut it compared to many of these other things.
im not arguing there isnt some cognitive dissonance to some of this, but if youre looking at the spectrum of not sbrt to full on SBRT, 25/5 rectal doesnt cut it compared to many of these other things.
We are a country divided. On race, on politics, on masking, on vaccines, on what is/isn't IMRT, on what is/isn't SBRT. WHO WILL UNITE US.I have tried in the past and failed to get preauth for sbrt 5 gy x 5 rectal. I figured we only get 90% of Medicare from this advantage plan, so why should the hospital not get something reasonable for the treatment.
In this calc, we will completely eliminate time corrections from consideration. This may actually be reasonable for very slowly dividing, very large Tpot tumors.Im sure lord wallrus can write us a thesis on the radbio of treating prostates 0.25-0.5 a day. How would you do it if you were asked lord wallrus?
I would also like to throw my vote behind 17/2.17/2 is fantastic.
I have zero clue why people don’t do it all the time
FL AZ CO California and Texas have nothing on upstate NY in terms of physician over fractionation and shenanigans. The hearing committee report is probably the most egregious thing I've ever heard of in our field and I've heard of some crazy stuff over the years. It's a wonder they didn't throw the guy in jailBut what I really took away from this thread:
