- Joined
- Aug 26, 2011
- Messages
- 1,555
- Reaction score
- 503

Also, out of 13,500 orthodontists, you are basing numbers out of only 107. I wasn't a stats major, but that just seems unpublishable!
I would also like to point out that the standard deviation for orthodontists was nearly pushing the average. That's a really large deviation.
Could you post a link to the original report?
Could you post a link to the original report?
<50-100 responses, don't know how much you can take from this report... and it shows with the SDs.
The one thing showing truth is OS > all
Above numbers are meaningless. Last year, I had to increase my hours since I lost two of my best referrals in town. They hired a new associate, and annual income almost dropped by half. You can see number of respondents are not significant either. They are many different factors involved and your income changes every year.
Above numbers are meaningless. Last year, I had to increase my hours since I lost two of my best referrals in town. They hired a new associate, and annual income almost dropped by half. You can see number of respondents are not significant either. They are many different factors involved and your income changes every year.
Ortho is starting to look less and less appealing when you start to consider you have to pay for residency.
Ortho is starting to look less and less appealing when you start to consider you have to pay for residency.
Why do you say thatOrthodontics is dying a slow death. In 5 or 10 years all the people going into it right now will wish they hadn't.
Why do you say that
Greater number of GPs taking on ortho to be able to pay off their student loansDecreasing overall income
Greater number of orthodontists
Larger and larger numbers of GPs doing orthodontics
Huge graduation debt loads
Giant corporate mills
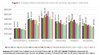
Here is a statistics from dental cpa in North East. I guess it is similar to the table above? But there are some experienced associate GPs who make $400k and there are some specialists making less than $200k... so I guess income range varies a lot
Money is not everything.
And note the median for ortho- huge discrepancy there. Means there are probably a few outliers making a huge amount compared to the others. Would love to see what the mean was if you took those out.
Median value is closer to what I think you're going to see in 5-10 years. There will be some lucky orthos that get to work for pediatric dental groups, but most of them are going to get screwed.
Orthodontics is dying a slow death. In 5 or 10 years all the people going into it right now will wish they hadn't.
Decreasing overall income
Greater number of orthodontists
Larger and larger numbers of GPs doing orthodontics
Huge graduation debt loads
Giant corporate mills
And note the median for ortho- huge discrepancy there. Means there are probably a few outliers making a huge amount compared to the others. Would love to see what the mean was if you took those out.
Median value is closer to what I think you're going to see in 5-10 years. There will be some lucky orthos that get to work for pediatric dental groups, but most of them are going to get screwed.
doesnt the ortho situation also apply to other specialties like OS? I feel like a lot of GPs are also doing the OS bread and butter dentistries like implants and wisdom teeth extractions. Hence, I assume the income for OS will be decreasing as well. Cant go into any speciality just for the money itself
Rosey: first and foremost, I am a big fan of yours and always follow your postings. If I may ask, why is California a tougher market?
However, from my understanding, California tends to be a tougher market in general. Many general dentists and specialists make less than the Median Salary in the US, at the expense of sunshine of course. Location will always remain an important factor.
Based on my own research (and the ADA's coincidentally), the Median Salaries do show some reflection.
Sent from my iPhone using SDN mobile
perhaps true, friend.Money is not everything.
Is it safe to assume that you talk to people that are struggling more financially than those you dont talk to?For what it's worth, most of the OMFS I've spoken with in the Northeast and California have been closer to that 1st quartile. The orthodontists I've spoken with in flyover country or the Southeast have been mostly at 3rd quartile or above. Peds dentists similar story with lots of saturation. It's really a tale of two professions, with many in the saturated high cost big cities living decent lives and the ones in the small and middle sized towns with less competition having a lot of economic success
For what it's worth, most of the OMFS I've spoken with in the Northeast and California have been closer to that 1st quartile. The orthodontists I've spoken with in flyover country or the Southeast have been mostly at 3rd quartile or above. Peds dentists similar story with lots of saturation. It's really a tale of two professions, with many in the saturated high cost big cities living decent lives and the ones in the small and middle sized towns with less competition having a lot of economic success
Is it safe to assume that you talk to people that are struggling more financially than those you dont talk to?
what's your thoughts on other specialites in real life? like endo, perio?
From what an OS told me, private practice OS don't work many hours. The OS having a worser lifestyle belief is due to the ones that work in hospitals. Private practice OS and endo's don't work many hours at all.Ortho here, a few years practicing. I read over this and I think it looks surprisingly accurate from a few different perspectives. OS and endo typically make far more than other specialists in my experience, at least on a per diem basis. However, what would really be interesting to know is how many days per year these people are working. I would guess that these numbers would be even more disparate if that was taken into consideration. I also believe the standard deviation or "spread" within ortho is huge. That is completely anecdotal, but I have worked in a number of different settings and closely with all types of specialists.
Lolworser
haha whoops
Yes, I know the grass is always greener....
Not a DA but my friend in Southeast Florida is doing well. He travels between offices (pediatric, general) and does cases. Makes a good living, travels with a nurse to assist. There is some competition from medical anesthesia doing the travelling gig but there seems to be a good market down here so everyone gets a nice share of the pie (I don't think its unheard of to do in the 250-300,000 range given the number of practices advertising "sedation" to attract clientele). As an OS I don't hire DAs usually, however for larger cases in the office (for example tentpole procedure for mandibular grafting from hip, full arch implants) I have hired anesthesia given intensive and long nature of these surgeries. Also, some of the DAs supplement/have their own general practices so that is another source of income.Anyone have any input for dentist anesthesiologists?
If you don’t use them, then the overhead shouldn’t be a problem. Many orthodontists in the past didn’t have any these expensive toys and they still provided excellent clinical results for their patients. It’s the painter and not the paintbrush.Overhead can also be a problem. CBCT, Invisalign, Suresmile etc all drive up overhead while fees are under pressure.
If you don’t use them, then the overhead shouldn’t be a problem. Many orthodontists in the past didn’t have any these expensive toys and they still provided excellent clinical results for their patients. It’s the painter and not the paintbrush.
It’s sad to see many ortho programs introducing the latest and the most expensive gadgets to their residents, instead of teaching them the basics such as handtracing the ceph, hand trimming the study models etc. And when they get out and work for a busy dental chain, they can’t handle the pressure because the chain offices lack these technologies. When they start their own office, they think that they have to have all these toys in order meet the standard of care and to attract patients. They think that in order to have a successful practice, they have to spend $500k to build it.
About 3 years ago, I moved my patients from a 3-op office to a larger 7-op office. The total cost for that move is $3k:
- Construction cost: $0. I share this new 7-op office with a GP owner. I pay him $1700/month in rent, which is the same as what I pay for the previous 3-op office.
- Pan/ceph machine: $10k. I bought a refurbished PC-1000 directly from Panoramic Corporation.
- X ray Developer: $600. I bought it used from a GP, who switched to digital xray.
- 4 Ortho chairs+ delivery units: $17k from Dome, Inc. The GP owner provides 3 chairs.
I sold the previous 3-op office to a new grad ortho for $25k. So the net cost for moving to a larger office is $3k. With a larger office, I can see twice as many patients in a day so I can work fewer days in a month.
In 2005, I spent $85k to build my first brand new office….and another $35k for 4 chairs and other equipments. It’s 100% paper chart…no computer, no management software, no need to deal with IT guys…..zero headache. The less I have to rely on the outside services (Invisalign, SureSmile, lab, tech supports, the sale reps etc), the more freedom I have in running my own practice.
In 2009, I bought an existing 1400sf 5-op office from a retiring ortho for $165k. Many orthos looked at the office but no one made an offer because it’s a dying office with only 140 active patients and the county was facing an economic recession. I bought it without any hesitation because it’s a lot cheaper than starting one from scratch.