- Joined
- Jun 20, 2005
- Messages
- 8,022
- Reaction score
- 2,816
- Points
- 5,251
- Attending Physician

can someone please explain to me why new grads put such small ETT's in pts these days?
Size matters: choosing the right tracheal tube - Farrow - 2012 - Anaesthesia - Wiley Online Librarycan someone please explain to me why new grads put such small ETT's in pts these days?
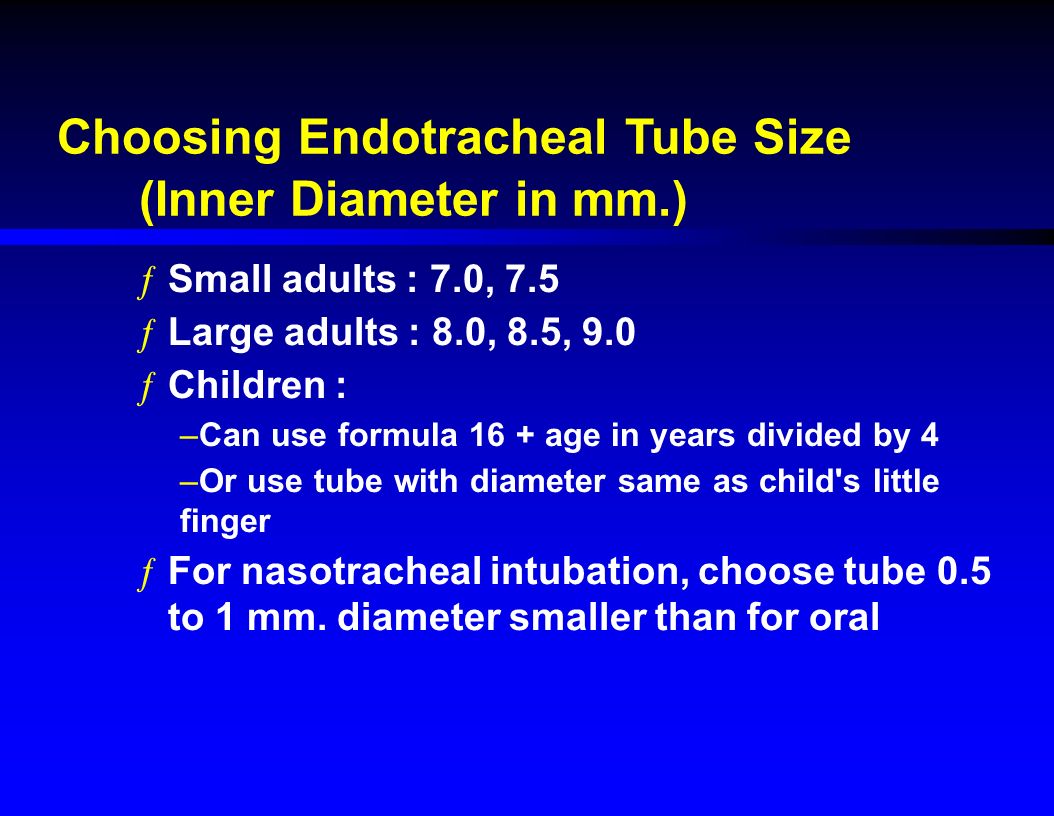
The larger the tube the smaller the risk of tracheal stenosis.This article suggests for ICU bound patients: 8.0 ETT for females, 9.0 for males... seems... quite large
smaller balls?can someone please explain to me why new grads put such small ETT's in pts these days?
His reasons for that (bronchial toilet, bronchoscopy, biofilm, less need for tube exchange, easier weaning) sound convincing.This article suggests for ICU bound patients: 8.0 ETT for females, 9.0 for males... seems... quite large
Defensive medicine.Can someone explain to me why garden-variety GERD *in and of itself* prompts people to put in an ETT?
(Also to give Bicitra and Reglan and Pepcid preop?)
6.5 malesHow small?
In my opinion a smaller ETT requires great cuff volume/pressure. Therefore great risk of sore throat.For regular cases I like the go smaller. I imagine less trauma/sore throat. Idk the data though.
In my opinion a smaller ETT requires great cuff volume/pressure. Therefore great risk of sore throat.
His reasons for that (bronchial toilet, bronchoscopy, biofilm, less need for tube exchange, easier weaning) sound convincing.

The larger the tube the smaller the risk of tracheal stenosis.
In my opinion a smaller ETT requires great cuff volume/pressure. Therefore great risk of sore throat.
I go 6.5 for females and 7 for males. If ICU bound then upsize to 8ish to facilitate bronchs/suction/etc.
I use 7s for everyone unless I expect postop ventilation. This is again one of those things that we can debate endlessly and doesn't make any difference in reality.
This is exactly what I do.
I don't see any reason to use a larger tube for a short case that's going to be extubated. My general vague philosophy is to use the smallest tube I can get away with. Particularly when it comes to double lumen tubes.
I think most sore throats are caused by laryngoscopes and the act of intubation, not endotracheal tubes per se. Gentle technique is probably the most important factor, and smaller tubes are sometimes technically easier to place.
I use 7s for everyone unless I expect postop ventilation. This is again one of those things that we can debate endlessly and doesn't make any difference in reality.
Large tubes were 9 mm (for men) and 8.5 mm (for women), and small tubes were 7 mm (for men) and 6.5 mm (for women). No lubricants were used. The sore-throat incidence in the group intubated with the large tubes was 48%, compared with 22% in the group intubated with the small tubes. No ventilatory difficulties were experienced as a result of using a small tube. Therefore, the use of smaller tubes has the distinct advantage of reducing the incidence of postoperative sore throat
Postoperative sore throat: cause, prevention and treatment - McHardy - 2002 - Anaesthesia - Wiley Online Library
7f/7.5m was standard in residency and what I've seen in two PP jobs since.I guess there is data to support me using smaller tubes haha. by small i mean 7f/7.5m
can someone please explain to me why new grads put such small ETT's in pts these days?
No it doesn't make a big difference. I just don't know where this training is coming from. It seems silly.Maybe you need to hire better grads?😉
Just kidding, but does it make that big of a difference?
This is exactly what I do.
I don't see any reason to use a larger tube for a short case that's going to be extubated. My general vague philosophy is to use the smallest tube I can get away with. Particularly when it comes to double lumen tubes.
I think most sore throats are caused by laryngoscopes and the act of intubation, not endotracheal tubes per se. Gentle technique is probably the most important factor, and smaller tubes are sometimes technically easier to place.
How are ppl sizing their DLTs? Those things are huge and seem to go down fine, which always reminds me that the human trachea can tolerate a big SLT, though it sure does look uncomfortable.
37 for everyone because it's hard to pass a bronchoscope through a 35.
Again, these new grads and their small... tubes. 😀37 for everyone because it's hard to pass a bronchoscope through a 35.
Any variation for gender or height?
I find it hard to believe that a 37 works for all your cases: i've had problems with tube length with 37sNot for me.
Again, these new grads and their small... tubes. 😀
It's cheaper than your Porsche.Nah, you guys are just overcompensating with your 8.5's.
Really? DLTs are super long. I don’t care if the Y of the DLT is in the mouth.I find it hard to believe that a 37 works for all your cases: i've had problems with tube length with 37s
It's cheaper than your Porsche.
I find it hard to believe that a 37 works for all your cases: i've had problems with tube length with 37s
Not long enough: when you have to hub it, they have a tendancy to move back out especially when moving to lateral.
I like 37 for women 39 for men 41 if really big.
New grad here. I have yet to see anyone pull out a 6.0 ETT for an adult female unless some form of airway obstruction is expected.
For routine cases, I put a 7.5 in everyone, male or female. Sometimes a 7.0 if they're really small. For cases where I expect the patient to stay intubated and go to ICU, 8.0 for everyone. No reason to go much larger than that.