- Joined
- Nov 21, 1998
- Messages
- 12,575
- Reaction score
- 6,977
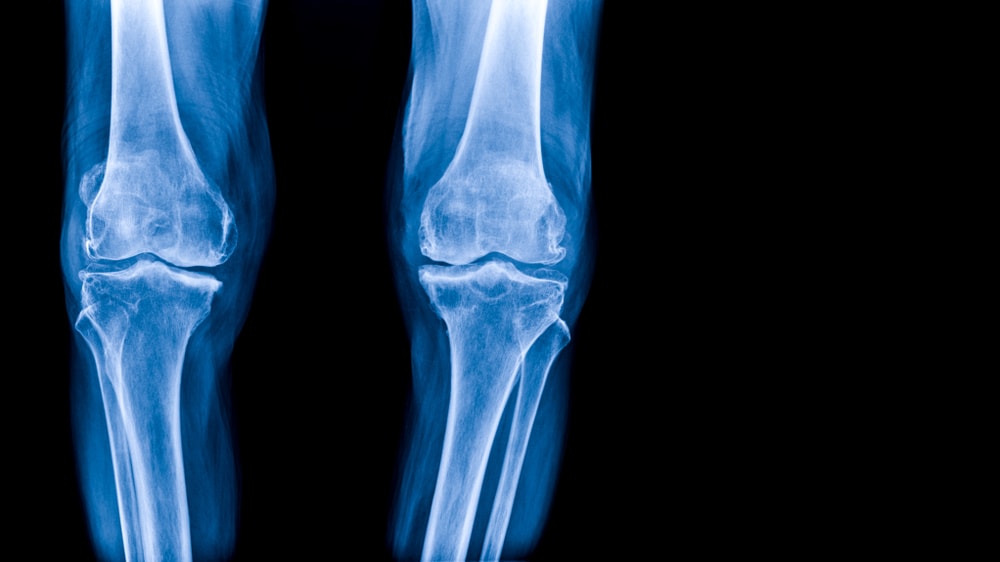
NSAIDs May Worsen Arthritis Inflammation
/PRNewswire/ -- Taking anti-inflammatory pain relievers like ibuprofen and naproxen for osteoarthritis may worsen inflammation in the knee joint over time,...
"For the study, 277 participants from the Osteoarthritis Initiative cohort with moderate to severe osteoarthritis and sustained NSAID treatment for at least one year between baseline and four-year follow-up were included in the study and compared with a group of 793 control participants who were not treated with NSAIDs. All participants underwent 3T MRI of the knee initially and after four years. Images were scored for biomarkers of inflammation. Cartilage thickness, composition and other MRI measurements served as noninvasive biomarkers for evaluating arthritis progression. The results showed no long-term benefit of NSAID use. Joint inflammation and cartilage quality were worse at baseline in the participants taking NSAIDs, compared to the control group, and worsened at four-year follow-up."