Lateral hip. L4?be specific about what part of the "hip" - anterior, lateral, posterior/buttock?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Right buttock pain down the leg, need management advice
- Thread starter CarabinerSD
- Start date

be specific about what part of the "hip" - anterior, lateral, posterior/buttock?
I’m assuming you’re gonna say: posterior L5 or S1, lateral L4, and anterior L3? TIA!
- Joined
- Nov 20, 2000
- Messages
- 1,785
- Reaction score
- 84
I guess you could say that certain lumbar dermatomes cross the region of the lateral hip.....I’m assuming you’re gonna say: posterior L5 or S1, lateral L4, and anterior L3? TIA!
- Joined
- Feb 1, 2005
- Messages
- 4,900
- Reaction score
- 1,884
Still nonspecific unless it is the occasional classic full spectrum of the dermatome/myotome. Any level can go to the buttock or lateral hip. L2, 3, 4 could be anywhere in the anterior or lateral thigh…. Or just glute.I guess you could say that certain lumbar dermatomes cross the region of the lateral hip.....
- Joined
- Oct 23, 2019
- Messages
- 72
- Reaction score
- 14
Appreciate all the input so far.Still nonspecific unless it is the occasional classic full spectrum of the dermatome/myotome. Any level can go to the buttock or lateral hip. L2, 3, 4 could be anywhere in the anterior or lateral thigh…. Or just glute.
I've performed an L5-S1 right ILESI today (good contrast pattern), if not helpful will repeat piriformis injection but with ultrasound instead since she keeps pointing to lower buttock for area of pain and under fluoro it's below SI joint...
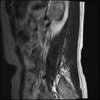
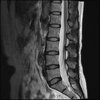
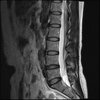
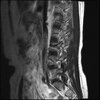
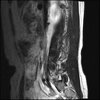
So here's the MRI L-spine for further analysis. I can only attach 10 images at a time.
Attachments
-
 LUMBAR SPINE WITHOUT CONTRAST 0001.jpg190.7 KB · Views: 55
LUMBAR SPINE WITHOUT CONTRAST 0001.jpg190.7 KB · Views: 55 -
 LUMBAR SPINE WITHOUT CONTRAST 0002.jpg189.3 KB · Views: 51
LUMBAR SPINE WITHOUT CONTRAST 0002.jpg189.3 KB · Views: 51 -
 LUMBAR SPINE WITHOUT CONTRAST 0003.jpg192.2 KB · Views: 54
LUMBAR SPINE WITHOUT CONTRAST 0003.jpg192.2 KB · Views: 54 -
 LUMBAR SPINE WITHOUT CONTRAST 0004.jpg193.7 KB · Views: 53
LUMBAR SPINE WITHOUT CONTRAST 0004.jpg193.7 KB · Views: 53 -
 LUMBAR SPINE WITHOUT CONTRAST 0005.jpg195.7 KB · Views: 55
LUMBAR SPINE WITHOUT CONTRAST 0005.jpg195.7 KB · Views: 55 -
 LUMBAR SPINE WITHOUT CONTRAST 0006.jpg195.2 KB · Views: 54
LUMBAR SPINE WITHOUT CONTRAST 0006.jpg195.2 KB · Views: 54 -
 LUMBAR SPINE WITHOUT CONTRAST 0007.jpg195.4 KB · Views: 56
LUMBAR SPINE WITHOUT CONTRAST 0007.jpg195.4 KB · Views: 56 -
 LUMBAR SPINE WITHOUT CONTRAST 0010.jpg196.2 KB · Views: 62
LUMBAR SPINE WITHOUT CONTRAST 0010.jpg196.2 KB · Views: 62 -
 LUMBAR SPINE WITHOUT CONTRAST 0009.jpg196.2 KB · Views: 59
LUMBAR SPINE WITHOUT CONTRAST 0009.jpg196.2 KB · Views: 59 -
 LUMBAR SPINE WITHOUT CONTRAST 0008.jpg194.6 KB · Views: 52
LUMBAR SPINE WITHOUT CONTRAST 0008.jpg194.6 KB · Views: 52
- Joined
- Oct 23, 2019
- Messages
- 72
- Reaction score
- 14
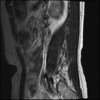
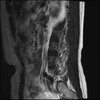
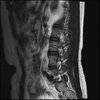
Sagital
Attachments



- Joined
- Oct 23, 2019
- Messages
- 72
- Reaction score
- 14
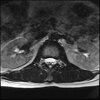
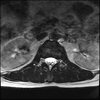
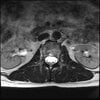
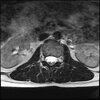
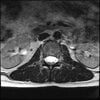
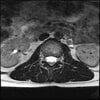
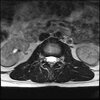
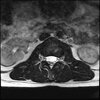
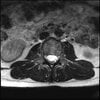
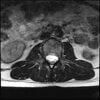
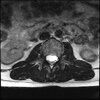
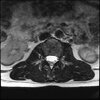
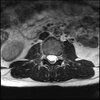
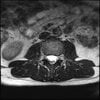
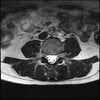
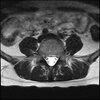
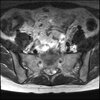
Axials
Attachments
-
 LUMBAR SPINE WITHOUT CONTRAST 0002.jpg184.1 KB · Views: 45
LUMBAR SPINE WITHOUT CONTRAST 0002.jpg184.1 KB · Views: 45 -
 LUMBAR SPINE WITHOUT CONTRAST 0001.jpg184.3 KB · Views: 40
LUMBAR SPINE WITHOUT CONTRAST 0001.jpg184.3 KB · Views: 40 -
 LUMBAR SPINE WITHOUT CONTRAST 0003.jpg186.6 KB · Views: 45
LUMBAR SPINE WITHOUT CONTRAST 0003.jpg186.6 KB · Views: 45 -
 LUMBAR SPINE WITHOUT CONTRAST 0004.jpg187.6 KB · Views: 45
LUMBAR SPINE WITHOUT CONTRAST 0004.jpg187.6 KB · Views: 45 -
 LUMBAR SPINE WITHOUT CONTRAST 0005.jpg187.9 KB · Views: 42
LUMBAR SPINE WITHOUT CONTRAST 0005.jpg187.9 KB · Views: 42 -
 LUMBAR SPINE WITHOUT CONTRAST 0006.jpg188.7 KB · Views: 44
LUMBAR SPINE WITHOUT CONTRAST 0006.jpg188.7 KB · Views: 44 -
 LUMBAR SPINE WITHOUT CONTRAST 0007.jpg189.4 KB · Views: 41
LUMBAR SPINE WITHOUT CONTRAST 0007.jpg189.4 KB · Views: 41 -
 LUMBAR SPINE WITHOUT CONTRAST 0008.jpg191 KB · Views: 44
LUMBAR SPINE WITHOUT CONTRAST 0008.jpg191 KB · Views: 44 -
 LUMBAR SPINE WITHOUT CONTRAST 0010.jpg190.8 KB · Views: 48
LUMBAR SPINE WITHOUT CONTRAST 0010.jpg190.8 KB · Views: 48 -
 LUMBAR SPINE WITHOUT CONTRAST 0009.jpg192 KB · Views: 50
LUMBAR SPINE WITHOUT CONTRAST 0009.jpg192 KB · Views: 50
- Joined
- Oct 23, 2019
- Messages
- 72
- Reaction score
- 14
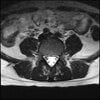
Axial
Attachments
-
 LUMBAR SPINE WITHOUT CONTRAST 0011.jpg188.7 KB · Views: 42
LUMBAR SPINE WITHOUT CONTRAST 0011.jpg188.7 KB · Views: 42 -
 LUMBAR SPINE WITHOUT CONTRAST 0012.jpg191.6 KB · Views: 40
LUMBAR SPINE WITHOUT CONTRAST 0012.jpg191.6 KB · Views: 40 -
 LUMBAR SPINE WITHOUT CONTRAST 0013.jpg192.2 KB · Views: 40
LUMBAR SPINE WITHOUT CONTRAST 0013.jpg192.2 KB · Views: 40 -
 LUMBAR SPINE WITHOUT CONTRAST 0017.jpg190.1 KB · Views: 53
LUMBAR SPINE WITHOUT CONTRAST 0017.jpg190.1 KB · Views: 53 -
 LUMBAR SPINE WITHOUT CONTRAST 0016.jpg189 KB · Views: 45
LUMBAR SPINE WITHOUT CONTRAST 0016.jpg189 KB · Views: 45 -
 LUMBAR SPINE WITHOUT CONTRAST 0015.jpg189.7 KB · Views: 42
LUMBAR SPINE WITHOUT CONTRAST 0015.jpg189.7 KB · Views: 42 -
 LUMBAR SPINE WITHOUT CONTRAST 0014.jpg190.6 KB · Views: 40
LUMBAR SPINE WITHOUT CONTRAST 0014.jpg190.6 KB · Views: 40 -
 LUMBAR SPINE WITHOUT CONTRAST 0018.jpg189 KB · Views: 40
LUMBAR SPINE WITHOUT CONTRAST 0018.jpg189 KB · Views: 40 -
 LUMBAR SPINE WITHOUT CONTRAST 0019.jpg194.9 KB · Views: 37
LUMBAR SPINE WITHOUT CONTRAST 0019.jpg194.9 KB · Views: 37 -
 LUMBAR SPINE WITHOUT CONTRAST 0020.jpg191.6 KB · Views: 41
LUMBAR SPINE WITHOUT CONTRAST 0020.jpg191.6 KB · Views: 41
- Joined
- Oct 23, 2019
- Messages
- 72
- Reaction score
- 14
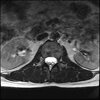
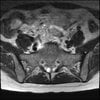
Axial
Attachments
-
 LUMBAR SPINE WITHOUT CONTRAST 0021.jpg190.3 KB · Views: 39
LUMBAR SPINE WITHOUT CONTRAST 0021.jpg190.3 KB · Views: 39 -
 LUMBAR SPINE WITHOUT CONTRAST 0024.jpg192.2 KB · Views: 47
LUMBAR SPINE WITHOUT CONTRAST 0024.jpg192.2 KB · Views: 47 -
 LUMBAR SPINE WITHOUT CONTRAST 0023.jpg192.9 KB · Views: 50
LUMBAR SPINE WITHOUT CONTRAST 0023.jpg192.9 KB · Views: 50 -
 LUMBAR SPINE WITHOUT CONTRAST 0022.jpg189 KB · Views: 48
LUMBAR SPINE WITHOUT CONTRAST 0022.jpg189 KB · Views: 48 -
 LUMBAR SPINE WITHOUT CONTRAST 0025.jpg193.4 KB · Views: 41
LUMBAR SPINE WITHOUT CONTRAST 0025.jpg193.4 KB · Views: 41 -
 LUMBAR SPINE WITHOUT CONTRAST 0026.jpg191.3 KB · Views: 43
LUMBAR SPINE WITHOUT CONTRAST 0026.jpg191.3 KB · Views: 43 -
 LUMBAR SPINE WITHOUT CONTRAST 0027.jpg191.1 KB · Views: 43
LUMBAR SPINE WITHOUT CONTRAST 0027.jpg191.1 KB · Views: 43 -
 LUMBAR SPINE WITHOUT CONTRAST 0028.jpg189.7 KB · Views: 49
LUMBAR SPINE WITHOUT CONTRAST 0028.jpg189.7 KB · Views: 49 -
 LUMBAR SPINE WITHOUT CONTRAST 0029.jpg192.9 KB · Views: 43
LUMBAR SPINE WITHOUT CONTRAST 0029.jpg192.9 KB · Views: 43 -
 LUMBAR SPINE WITHOUT CONTRAST 0030.jpg195.1 KB · Views: 41
LUMBAR SPINE WITHOUT CONTRAST 0030.jpg195.1 KB · Views: 41
- Joined
- Oct 23, 2019
- Messages
- 72
- Reaction score
- 14
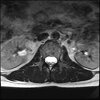
Axial
Attachments
-
 LUMBAR SPINE WITHOUT CONTRAST 0033.jpg195.9 KB · Views: 45
LUMBAR SPINE WITHOUT CONTRAST 0033.jpg195.9 KB · Views: 45 -
 LUMBAR SPINE WITHOUT CONTRAST 0032.jpg193 KB · Views: 48
LUMBAR SPINE WITHOUT CONTRAST 0032.jpg193 KB · Views: 48 -
 LUMBAR SPINE WITHOUT CONTRAST 0031.jpg192.9 KB · Views: 46
LUMBAR SPINE WITHOUT CONTRAST 0031.jpg192.9 KB · Views: 46 -
 LUMBAR SPINE WITHOUT CONTRAST 0034.jpg196.3 KB · Views: 57
LUMBAR SPINE WITHOUT CONTRAST 0034.jpg196.3 KB · Views: 57 -
 LUMBAR SPINE WITHOUT CONTRAST 0035.jpg196.1 KB · Views: 46
LUMBAR SPINE WITHOUT CONTRAST 0035.jpg196.1 KB · Views: 46 -
 LUMBAR SPINE WITHOUT CONTRAST 0036.jpg197.2 KB · Views: 56
LUMBAR SPINE WITHOUT CONTRAST 0036.jpg197.2 KB · Views: 56 -
 LUMBAR SPINE WITHOUT CONTRAST 0040.jpg196.4 KB · Views: 58
LUMBAR SPINE WITHOUT CONTRAST 0040.jpg196.4 KB · Views: 58 -
 LUMBAR SPINE WITHOUT CONTRAST 0039.jpg197.2 KB · Views: 53
LUMBAR SPINE WITHOUT CONTRAST 0039.jpg197.2 KB · Views: 53 -
 LUMBAR SPINE WITHOUT CONTRAST 0038.jpg197.8 KB · Views: 45
LUMBAR SPINE WITHOUT CONTRAST 0038.jpg197.8 KB · Views: 45 -
 LUMBAR SPINE WITHOUT CONTRAST 0037.jpg198.2 KB · Views: 54
LUMBAR SPINE WITHOUT CONTRAST 0037.jpg198.2 KB · Views: 54
- Joined
- Oct 23, 2019
- Messages
- 72
- Reaction score
- 14


- Joined
- Apr 28, 2010
- Messages
- 1,313
- Reaction score
- 1,385
Even less impressive than the report
D
deleted875186
Agreed, lumbar spine is mild, doesn’t explain the pain.
- Joined
- Apr 2, 2010
- Messages
- 375
- Reaction score
- 134
Sacral tarlov cysts? Could explain pain.
- Joined
- May 30, 2005
- Messages
- 21,258
- Reaction score
- 12,375
NO it can’tSacral tarlov cysts? Could explain pain.
D
deleted875186
I stand by what I said earlier. Try lumbar facets. Would also reconsider the hip joint.
- Joined
- Apr 2, 2010
- Messages
- 375
- Reaction score
- 134
lol not falling for thisNO it can’t
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
Tarlov cysts do not hurt.lol not falling for this
OP - Become okay telling ppl you can't fix them or take away all of their problems.
This pt isn't going to get better with your injxns and she'll prob look back in 24 months and be pissed you kept sticking her.
- Joined
- Dec 13, 2005
- Messages
- 5,318
- Reaction score
- 3,597
Normal mri
I do think it's the cyst. If all of it doesn't help, ask an IR to do a cyst aspiration and injection of fibrin. That's a right S2 cyst correct?

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
Treatment of 213 Patients with Symptomatic Tarlov Cysts by CT-Guided Percutaneous Injection of Fibrin Sealant
This cohort study assesses outcomes in patients who underwent CT-guided aspiration and injection of sacral Tarlov cysts at Johns Hopkins Hospital from 2003–2013. A total of 289 cysts were treated in 213 consecutive patients, with 83% followed ...
www.ncbi.nlm.nih.gov
- Joined
- Apr 2, 2010
- Messages
- 375
- Reaction score
- 134
Prove itTarlov cysts do not hurt.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
How?Prove it
I've never heard of Tarlov cysts causing pain.
Last edited:
- Joined
- Apr 2, 2010
- Messages
- 375
- Reaction score
- 134
Thank youHow?
- Joined
- May 30, 2005
- Messages
- 21,258
- Reaction score
- 12,375
How do you account for the 174 who declined treatments from a statistical standpoint? BOCF.I do think it's the cyst. If all of it doesn't help, ask an IR to do a cyst aspiration and injection of fibrin. That's a right S2 cyst correct?
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
but a perineural cyst is different than a tarlov cyst right?How do you account for the 174 who declined treatments from a statistical standpoint? BOCF.
View attachment 369855
- Joined
- May 30, 2005
- Messages
- 21,258
- Reaction score
- 12,375
I don't think so for this study. Will have to relook.but a perineural cyst is different than a tarlov cyst right?
- Joined
- Apr 2, 2010
- Messages
- 375
- Reaction score
- 134
I’ve had at least one patient in last year that I’ve narrowed down to this. Buttock pain only.How?
I've never heard of Tarlov cysts causing pain.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
How exactly did you do that?I’ve had at least one patient in last year that I’ve narrowed down to this. Buttock pain only.
This discussion has come up repeatedly. I was always taught they don't hurt. Truthfully, I don't know why they would hurt either.
It's pain, not diabetes.
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
Honestly I think they’re like anything else in the spine, annular tears, disc protrusions, spondylosis. In the right setting and with enough inflammation they can be painful but typically are asymptomaticHow exactly did you do that?
This discussion has come up repeatedly. I was always taught they don't hurt. Truthfully, I don't know why they would hurt either.
It's pain, not diabetes.
In the right setting and with enough inflammation? What are you even talking about? The right setting is never.Honestly I think they’re like anything else in the spine, annular tears, disc protrusions, spondylosis. In the right setting and with enough inflammation they can be painful but typically are asymptomatic

- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
Tbone you’ve established your ignorance before. No need to explain buddyIn the right setting and with enough inflammation? What are you even talking about? The right setting is never.
D
deleted875186
I could be convinced cysts cause symptoms of IR drains a cyst and it relieves their symptoms. But excluding other causes doesn’t convince me the cysts are symptomatic, plenty of people have pain symptoms without a clear cause.In the right setting and with enough inflammation? What are you even talking about? The right setting is never.
Cmon @clubdeac relax a little bit. If you want to start a new thread called “ the ignorance of Tboned” go ahead. But re: this thread, I’m always willing to learn. Explain what you’re talking about, I’m interested to hear your thoughts on the inflammatory component or a Tarlov cyst. How are you determining that? It’s not an apples to apples comparison with annular tears and other pathology you hinted at.Tbone you’ve established your ignorance before. No need to explain buddy
I don't think of Tarlov cysts as necessarily inflammatory. There was some early postulations about inflammation playing a role in their creation, but I don't know if they really cause inflammation. I do see that they are capable of generating a great deal of pressure. As you look for them more, you'll see cysts that cause remodeling of the bone around them from outward pressure. It's not unreasonable to me then that the pressure causes a neuropraxia of a nerve root inside or outside the cyst. Drainage by IR or an aggressive pain doc allows one to verify that this is the generator. That fibrin injection thing may work sometimes, but I've seen mixed results. I haven't seen a surgeon willing to work on them.
I'm not sure I get the BOCF? Google says baseline-observation-carried-forward which might make sense if you're looking at this like a RCT for ITT, but this is a retrospective case series.
I interpret this as a subgroup they selected for have good results with drainage/fibrin patching, but they may have weeded out a lot of cases that they didn't think would have good results. I would love to hear more about that population too and understand the selection criteria.
I think of that as "Patient Selection"How do you account for the 174 who declined treatments from a statistical standpoint? BOCF.
I'm not sure I get the BOCF? Google says baseline-observation-carried-forward which might make sense if you're looking at this like a RCT for ITT, but this is a retrospective case series.
I interpret this as a subgroup they selected for have good results with drainage/fibrin patching, but they may have weeded out a lot of cases that they didn't think would have good results. I would love to hear more about that population too and understand the selection criteria.
- Joined
- May 30, 2005
- Messages
- 21,258
- Reaction score
- 12,375
208 had cysts and were the selected patients. 34 had direct surgery referral and 174 said no thanks. Lets say every one of those 208 was treated and had excellent results. Now lets say all 208 had terrible results. It would completely change the outcomes. They only treated 213.I don't think of Tarlov cysts as necessarily inflammatory. There was some early postulations about inflammation playing a role in their creation, but I don't know if they really cause inflammation. I do see that they are capable of generating a great deal of pressure. As you look for them more, you'll see cysts that cause remodeling of the bone around them from outward pressure. It's not unreasonable to me then that the pressure causes a neuropraxia of a nerve root inside or outside the cyst. Drainage by IR or an aggressive pain doc allows one to verify that this is the generator. That fibrin injection thing may work sometimes, but I've seen mixed results. I haven't seen a surgeon willing to work on them.
I think of that as "Patient Selection"
I'm not sure I get the BOCF? Google says baseline-observation-carried-forward which might make sense if you're looking at this like a RCT for ITT, but this is a retrospective case series.
I interpret this as a subgroup they selected for have good results with drainage/fibrin patching, but they may have weeded out a lot of cases that they didn't think would have good results. I would love to hear more about that population too and understand the selection criteria.
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
So we know inflammation is a necessary component to experience pain in spinal stenosis, facet arthritis, discogenic lbp and particularly radicular pain. You need two things to experience pain in these scenarios, some structural or anatomical pathology AND inflammation. If you take one of these away, the patient typically won’t experience pain regardless of the MRI findings. There are studies showing this.Cmon @clubdeac relax a little bit. If you want to start a new thread called “ the ignorance of Tboned” go ahead. But re: this thread, I’m always willing to learn. Explain what you’re talking about, I’m interested to hear your thoughts on the inflammatory component or a Tarlov cyst. How are you determining that? It’s not an apples to apples comparison with annular tears and other pathology you hinted at.
I’ve seen multiple patients with asymptomatic tarlov cysts as well those where nothing else explains their pain other than the tarlov cyst. In those cases I presume the cyst is pressing on pain generating structures. However based on what we know about spinal pathology, there is likely an inflammatory component. I don’t know that but am rather extrapolating from what we know about other spinal pathologies
Last edited:
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
I’m talking about typical spinal pain, not CRPS, central pain syndrome, fibromyalgia, phantom limb pain, chronic pelvic pain etc.Pain does not require an anatomical basis.
- Joined
- Jun 16, 2021
- Messages
- 2,358
- Reaction score
- 2,597
Me tooI’m talking about typical spinal pain, not CRPS, central pain syndrome, fibromyalgia, phantom limb pain, chronic pelvic pain etc.
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
technically, you do not require anything anatomic to experience pain. see fibromyalgia (at least based on what we know about it now)So we know inflammation is a necessary component to experience pain in spinal stenosis, facet arthritis, discogenic lbp and particularly radicular pain. You need two things to experience pain, some structural or anatomical pathology AND inflammation. If you take one off these away, the patient typically won’t experience pain regardless of the MRI findings. There are studies showing this.
I’ve seen multiple patients with asymptomatic tarlov cysts as well those where nothing else explains their pain other than the tarlov cyst. In those cases I presume the cyst is pressing on pain generating structures. However based on what we know about spinal pathology, there is likely an inflammatory component. I don’t know that but am rather extrapolating from what we know about other spinal pathologies
pain is a subjective experience.
and when i look at MRI scans for failed back syndrome, im not seeing a lot of inflammation. even facet arthropathy - is that were purely inflammation, then steroidal therapy would be the mainstay and only treatment, right?
tarlov cysts can cause pain, but it not the cyst itself. it is when a huge cyst scallops out the sacrum or compresses S1 or S2. this is exceptionally rare. maybe 2 cases in 15 years. ive diagnosed them on EMG. surgery is +/-. they shouldt be dismissed outright, but id say 99% of the time they mean nothing
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
I guess no one read what I wrote. Oh welltechnically, you do not require anything anatomic to experience pain. see fibromyalgia (at least based on what we know about it now)
pain is a subjective experience.
and when i look at MRI scans for failed back syndrome, im not seeing a lot of inflammation. even facet arthropathy - is that were purely inflammation, then steroidal therapy would be the mainstay and only treatment, right?
“So we know inflammation is a necessary component to experience pain in spinal stenosis, facet arthritis, discogenic lbp and particularly radicular pain.”
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
yes we did.
so why do you feel that inflammation is a necessary component to experience pain from the 4 conditions you state?
you state there are studies. can you post them?
so why do you feel that inflammation is a necessary component to experience pain from the 4 conditions you state?
you state there are studies. can you post them?
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
Studies are from fellowship as are the text book references. I could try and find them but this is like finding the study that shows seat belts save lives, not really necessary. Again I’m talking about the 95% of scenarios with lumbar radic, spinal stenosis, facet arthritis etcyes we did.
so why do you feel that inflammation is a necessary component to experience pain from the 4 conditions you state?
you state there are studies. can you post them?
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
how often do we see edema or elevated ESR in these patients with arthritic spines?
then again, maybe you are conflating the presence of inflammatory cytokines - substance P, histamines - in the chemical milieu contributing to neuropathic pain in your definition of inflammation....
then again, maybe you are conflating the presence of inflammatory cytokines - substance P, histamines - in the chemical milieu contributing to neuropathic pain in your definition of inflammation....
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
I’m not conflating anything. But yes that’s exactly what I’m talking about. Those are inflammatory mediators and although they may not directly raise ESR or CRP, that doesn’t mean there isn’t inflammation present. I mean cmon, we all prescribe NSAIDs for inflammation everyday. Most all of these patients have normal ESRs. Does that mean we’re not treating inflammation or we’re conflating something? This really shouldn’t be difficult or controversialhow often do we see edema or elevated ESR in these patients with arthritic spines?
then again, maybe you are conflating the presence of inflammatory cytokines - substance P, histamines - in the chemical milieu contributing to neuropathic pain in your definition of inflammation....
- Joined
- Oct 7, 2011
- Messages
- 14,664
- Reaction score
- 5,967
inflammatory mediators =/= inflammation.
huge difference.
which is why steroid injections dont work for facet arthritis or degenerative spinal stenosis with neurogenic claudication.
and ive stopped prescribing NSAID for the types of conditions you describe.
why?
they dont work.
because it is not inflammation that is driving their pain.
huge difference.
which is why steroid injections dont work for facet arthritis or degenerative spinal stenosis with neurogenic claudication.
and ive stopped prescribing NSAID for the types of conditions you describe.
why?
they dont work.
because it is not inflammation that is driving their pain.
- Joined
- Aug 16, 2007
- Messages
- 5,386
- Reaction score
- 2,526
I give up with you. Steroid injections work remarkably well in the short term (~3 months) for spinal stenosis and facet arthritis. You must be doing them wrong.inflammatory mediators =/= inflammation.
huge difference.
which is why steroid injections dont work for facet arthritis or degenerative spinal stenosis with neurogenic claudication.
and ive stopped prescribing NSAID for the types of conditions you describe.
why?
they dont work.
because it is not inflammation that is driving their pain.
I'd be interested in hearing your theory regarding the pathophysiology of facet mediated pain, spinal stenosis, discogenic lbp, painful radiculopathy etc. What is your understanding of nociception?
And when I refer to inflammation I do mean substance P, IL-6, cytokines, TNF-alpha, PLA2 and on and on...
- Joined
- May 30, 2005
- Messages
- 21,258
- Reaction score
- 12,375
Steroid injections do not work for facet arthritis.I give up with you. Steroid injections work remarkably well in the short term (~3 months) for spinal stenosis and facet arthritis. You must be doing them wrong.
I'd be interested in hearing your theory regarding the pathophysiology of facet mediated pain, spinal stenosis, discogenic lbp, painful radiculopathy etc. What is your understanding of nociception?
And when I refer to inflammation I do mean substance P, IL-6, cytokines, TNF-alpha, PLA2 and on and on...