- Joined
- Aug 14, 2016
- Messages
- 645
- Reaction score
- 930
Psai's caustic but hilarious posts are one of the best things about SDN, tbh.

Lol premeds... I guess that h8ers gonna sip h8torade am I right?
Lol Psai isn’t a pre-med
What?Then why would he be taking gen chem? For the fun in it?
Tbf, you do have control over what field you choose specialize (presuming you have the qualifications to match). While I think primary care will continue to be a good job, and that midlevels won't replace physician experts, the fact that physicians will have compete with independently practicing NPs does discourage me from pursuing it. Many patients would be willing to pay more to see a physician, but it's a question of how much more. Midlevels, who would be happy to work for 120k a year, will put pressure on primary care physician salary. Since every insurance plan compensates specialists more than PC physicians and midlevels are less able to compete with specialists, I would advise med students to pursue a speciality unless they have a burning passion for primary care.
As for radiology, AI may decrease the demand for radiologists because its improves their productivity, but there will always be a need for physician experts in medical imaging. AI will replace some of what radiologists do, decreasing their workload, but not all of it. Don't pursue it just for the pay, which doesn't seem to be that relatively high anymore, but if you're interested in medical imaging and like the other aspects of the job, I think it's a great choice.
Are you an AMA member? Have you ever shown up to a House of Delegates meeting? My guess is no. Mid level encroachment has been a hot topic at meetings for the past two years at least. At any rate, your state medical society has more clout in that arena. Don’t just complain. Get involved!Uhhhh physicians are already being let go by hospital admin and replaced with NPs at many places. The AANP lobby is only getting stronger, not weaker, whereas the AMA doesn't do zilch. You need to open your eyes if you don't think that this is an issue for physicians in the future.
“I’m going into primary care for the money!” Said no one everPersonally I am interested in primary care and so this report is disheartening. Just don't do it for the money.
Yep. My office has me and one NP. I'm seeing 12-15 patients/day (I only started back in May). The NP, who has been here since February, is lucky if she gets 6 appointments in a day. At least 3-5 patients/week have switched from her to me since I started.If anything I feel like PC physicians are pretty well-insulated from mid-levels. For routine office visits, the vast majority of people when asked, they'd still prefer to see a DOCTOR over a mid-level. For the non-urgent stuff, some even are willing to wait for weeks to see their doctors. When I was on my Family Medicine rotation, one of my attendings recently moved to the area to join the hospital practice, many of his old patients would drive an hour and a half to see him, a few even switched insurance carriers. Obviously there are the few special ones out there who'd prefer to see their favorite NP/PA or whatever over a doctor and be very vocal about it on fb/online. There is no shortage of patients out there and the demand for PC docs is HUGE.
Yeah I had a solo me-owned practice for a few years. While the freedom was nice, having to worry about lease payments, revenue, HR stuff all sucked. I'd much rather just see patients knowing I'll earn slightly less doing so than I would on my own but not having to run a business.this thread reminds me why i quit sdn. the old-guard members get away with making personal attacks and everyone parrots the same head-in-the-sand nonsense.
congratulations, you are the hospital-admin-serving slaves (or are positioning yourself to be, if you're not an attending yet) you never thought youd become.
You must be new here...Then why would he be taking gen chem? For the fun in it?
Are you an AMA member? Have you ever shown up to a House of Delegates meeting? My guess is no. Mid level encroachment has been a hot topic at meetings for the past two years at least. At any rate, your state medical society has more clout in that arena. Don’t just complain. Get involved!
I'm curious to see how this pans out long term for patients finding out they need specialist they can't afford without insurance leading to preemptive insurance coverage plus membership fees for the DPC. It's hard to convince people, especially older ones that it's a win for them.On a serious note, direct primary care could be the wave of the future...there will be a rough transition from fee-for-service but you eliminate overhead from dealing with 3rd party payers which is the biggest obstacle and operate your practice the way you see fit - essentially back to being doctors in every sense
That's an easy one.I'm curious to see how this pans out long term for patients finding out they need specialist they can't afford without insurance leading to preemptive insurance coverage plus membership fees for the DPC. It's hard to convince people, especially older ones that it's a win for them.
Sent from my Pixel XL using SDN mobile
Right, but does is this reduction enough to actually as a whole cost less or break even? From my understanding, which is admittedly weak, primary care cost are a small amount of the cost insurance companies cover and thus not much savings to be had by it's removal.That's an easy one.
If insurance stops covering primary care, it becomes cheaper (or you get better coverage for your money).
Plus most specialists aren't that expensive either if you offer to pay cash.
My experience from running a DPC practice and contracting with local employers/local insurance is that it does. You see savings in a number of ways:Right, but does is this reduction enough to actually as a whole cost less or break even? From my understanding, which is admittedly weak, primary care cost are a small amount of the cost insurance companies cover and thus not much savings to be had by it's removal.
Sent from my Pixel XL using SDN mobile
That sounds awesome. Ive known about DPC and really liked what I've seen of it. We have one that just opened up near us that seems pretty solid. It does beg the question though... Why isn't everyone utilizing these style practices already, and why did you leave DPC?My experience from running a DPC practice and contracting with local employers/local insurance is that it does. You see savings in a number of ways:
Fewer referrals. This isn't universally true, but lots of stuff gets referred out because there isn't time to manage it properly. DPC tends to fix that. I don't refer out often these days in FFS, but it is more than I did in DPC.
Cost savings. Most DPC practices have pretty crazy prices for meds/labs. For example: I picked up a diflucan at the drug store 2 weeks ago. Cost me $12 using insurance (my insurance paid out $10, I paid $12). Through my old DPC practice, that would have been $2. At my yearly physical, I get a CMP and lipids since I'm on crestor. Insurance paid around $50, I paid about the same. At my old DPC practice, those tests together would have been $11.
Decreased utilization. We all know that lots of people go to the doctor with minor stuff. Most DPC offers e-mail/text access. I can't tell you how many patients would shoot me a quick message (often times with a picture if it was a rash or injury) and I was able to manage whatever it was without an office visit.
Generally speaking, switching to DPC means taking a hit to your income and usually having to either get a loan or put your own money up for start-up costs. Doctors are not known for taking risks. Plus there's the whole "running the business" aspect which most doctors don't enjoy. Payroll, OSHA/health department rules, taxes, insurance, utilities, and so on.That sounds awesome. Ive known about DPC and really liked what I've seen of it. We have one that just opened up near us that seems pretty solid. It does beg the question though... Why isn't everyone utilizing these style practices already, and why did you leave DPC?
Sent from my Pixel XL using SDN mobile
Nah we should be in DC fighting this stuff. We chill too much!
I disagree with this one. Look at what is happening to EKGs. Ive seen many cardiologists just glance at ekg for like 2 seconds and put their name on it. Machine reading has gotten really good for simple stuff.
The same thing can happen for radiology. Put AI in for simple stuff first. I imagine the government will be for it if you tell them it lowers cost since healthcare cost is going nuts.
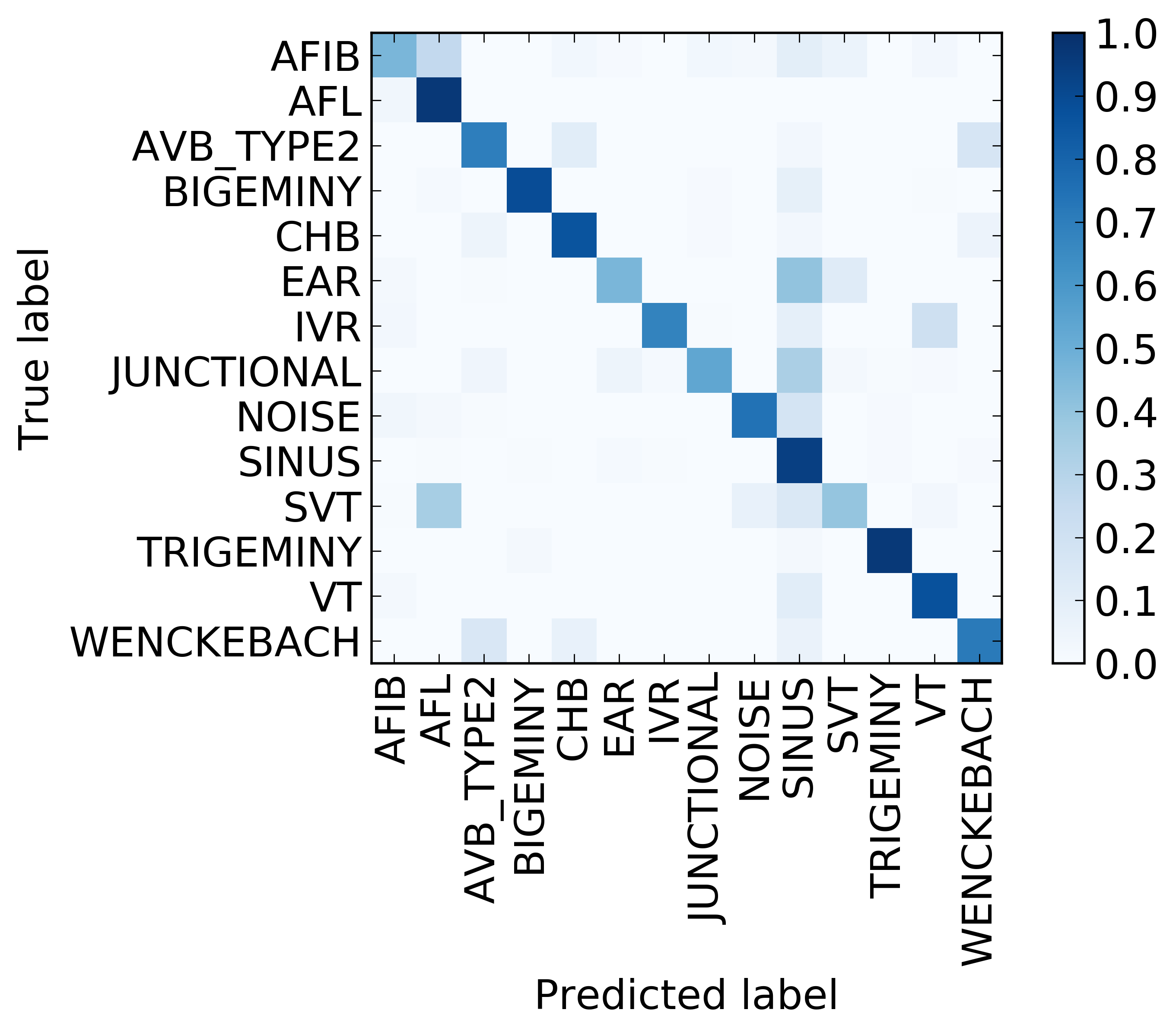
We develop an algorithm which exceeds the performance of board certified cardiologists in detecting a wide range of heart arrhythmias from electrocardiograms recorded with a single-lead wearable monitor. We build a dataset with more than 500 times the number of unique patients than previously studied corpora. On this dataset, we train a 34-layer convolutional neural network which maps a sequence of ECG samples to a sequence of rhythm classes. Committees of board-certified cardiologists annotate a gold standard test set on which we compare the performance of our model to that of 6 other individual cardiologists. We exceed the average cardiologist performance in both recall (sensitivity) and precision (positive predictive value).
Officially that is true, but I am on the payroll now for orientation... getting my first paycheck first week of July.True, but I don't think anyone is actually working as a new intern just yet. If memory serves, the start date is July 1.
My program was set up the same way, During orientation as there were three active classes of residents and I was not among them we weren't really considered interns. Once we started work and the previous third years were no longer working, we were.Officially that is true, but I am on the payroll now for orientation... getting my first paycheck first week of July.
I'm curious to see how this pans out long term for patients finding out they need specialist they can't afford without insurance leading to preemptive insurance coverage plus membership fees for the DPC. It's hard to convince people, especially older ones that it's a win for them.
Sent from my Pixel XL using SDN mobile
That's when insurance kicks in and what it's designed to doSome DPC's contract with specialists and that fee is included in the patient's "membership" fee which is still cheaper than holding insurance. Still the question remains what happens when the pt needs to be admitted and/or procedures are necessary
When the Boomers start all dying, then we might see demand go down but we've got about 15-20 years until the middle of that group hits average life expectancy.
I'm a late Millennial already on a statin (not overweight though you fat-shaming bastard!)Well as an older Millenial in my 30s, all the people I went to high school with are now fat or getting fat, so by the time the boomers die off, my generation will all need statins and insulin.
I'm a late Millennial already on a statin (not overweight though you fat-shaming bastard!)
Why are you assuming things about me and my post? I said the AMA doesn't do anything and they really don't. We can talk about the issue until the next decade but this problem isn't fixing itself. We need strong lobbying, we need funding for anti-media campaigns, we need a strong push for publicity on this issue. The AANP is literally pushing this issue down everyone's throats and running attack campaigns against us in order to achieve what they want. They know how to really fight for their constituents. While I can dislike what they're doing, I can respect how much they're actually getting done. Compared to that, the AMA is literally doing NOTHING.
Sorry for making an unfounded assumption about you.
I assumed you were not a dues-paying member since you didn't seem to be aware of the efforts the AMA has been making in this arena. Resolution 214, passed during at the Interim meeting last November, called on the AMA to "effectively oppose continual, nationwide efforts to grant independent practice to non-physician practictioners." An organization is only as powerful as its members. Only 25% of practicing physicians belong to the AMA. If physicians wanted to unite to fight a common cause, you would think there'd be more of an effort to set aside differences and join the AMA. The AMA wages its own media campaigns that have ramped up in recent years if you've been paying attention. They're still the most powerful physician lobby in the U.S., and they comment on every major medical (and even non-medical: see the recent Annual Meeting press releases) issue in the press. What's your metric to compare the success of AANP's lobby to that of the AMA? The majority of states still do not allow NPs to practice independently.
Again, your state medical society in the place to concentrate your effort to have the most immediate effects on NP regulations. The AMA has representatives from state societies attend and vote on policy at their meetings, but state societies are funded independently, as far as I know.
I dont agree. I'm a small business owner and having seen the logistics behind a medical practice... it seriously is not that hard. If you're just somewhat mediocre at business you should be able to do well. What it comes down to is whether or not you're willing to put in the extra effort/mental energy etc. That's the key distinguishing factor.Yeah I had a solo me-owned practice for a few years. While the freedom was nice, having to worry about lease payments, revenue, HR stuff all sucked. I'd much rather just see patients knowing I'll earn slightly less doing so than I would on my own but not having to run a business.
Here's a tip: most doctors suck at business. The majority of the time, we make more being employed even with admin taking some of the revenue from us.
I didn't say it was hard. I said its extra work that sucked and that, generally speaking, doctors aren't good at it.I dont agree. I'm a small business owner and having seen the logistics behind a medical practice... it seriously is not that hard. If you're just somewhat mediocre at business you should be able to do well. What it comes down to is whether or not you're willing to put in the extra effort/mental energy etc. That's the key distinguishing factor.
reimbursement has a lot more to do with it. Child neurologists are not making millions of dollars due to low supply and high demand, nor are dual med -ped or med -emergency physicians. If you do a procedure that reimburses well and you can crank a lot of them you are going to get paid a lot.Thats a really good point. Reimbursement does have a lot do with it, but thats not to say that supply and demand has nothing to do with it. As cited earlier it takes time for salaries to react to the supply/demand curve.
reimbursement has a lot more to do with it. Child neurologists are not making millions of dollars due to low supply and high demand, nor are dual med -ped or med -emergency physicians. If you do a procedure that reimburses well and you can crank a lot of them you are going to get paid a lot.
Actually this point is even contentious. Look up Supply driven demand. It is a huge driver of the difference in procedure rates in areas where there is an overabundance of proceduralists.I never said otherwise, but it would be illogical to not recognize the role supply/demand plays. Although extreme, if you can't find a job then you can't do any procedures.
Actually this point is even contentious. Look up Supply driven demand. It is a huge driver of the difference in procedure rates in areas where there is an overabundance of proceduralists.
So how long do members here predict until there is an oversaturation of MLPs? Just curious what everyone's thoughts are are on this.
So how long do members here predict until there is an oversaturation of MLPs? Just curious what everyone's thoughts are are on this.
Also keep in mind that over the next two decades, Baby Boomer docs will be retiring or dying off in droves.Future of primary care is excellent, more population, more sick people, everyone living longer. IF you are interested in money, future of primary care and medicine in general is in peril because physicians and their prescription pads will become more and more a vehicle rather than an end-all be-all towards getting care. Look at telemedicine and advances in AI. There will be more computer doing diagnosis and less human interaction and less ability to make money. If you like the patient side, that will always be there. We all need a person who cares!!!
Follow me for more posts like these!
AB
Which physicians have jobs that are easy to do when your 55 and which ones have jobs that are hard to do when your 55?