- Joined
- Apr 21, 2011
- Messages
- 3,775
- Reaction score
- 9,653
- Points
- 7,311
NEED more scarb CONTENT!!!!

I believe you 100% and without any hesitation.All of my fellow PGY-5s I have talked with - including those at my program and other programs - received offers for jobs that were not publicly advertised or posted. This is of course anecdotal, but nonetheless a large n. Again, we all have jobs, not fellowships, in highly desirable cities.
Just trying to introduce a dose of reality!
The only reason I'm replying is to make sure to stamp out the fake news.
So how do you think this is possible. Prostate cancer is, as you know, the most common cancer in men. Number of new cases per year has dropped by ~33% over the last 10y, and we are about 25y out from the advent of PSA testing. The incidence held steady as you can see for many years after this advent (1990-95 time frame).
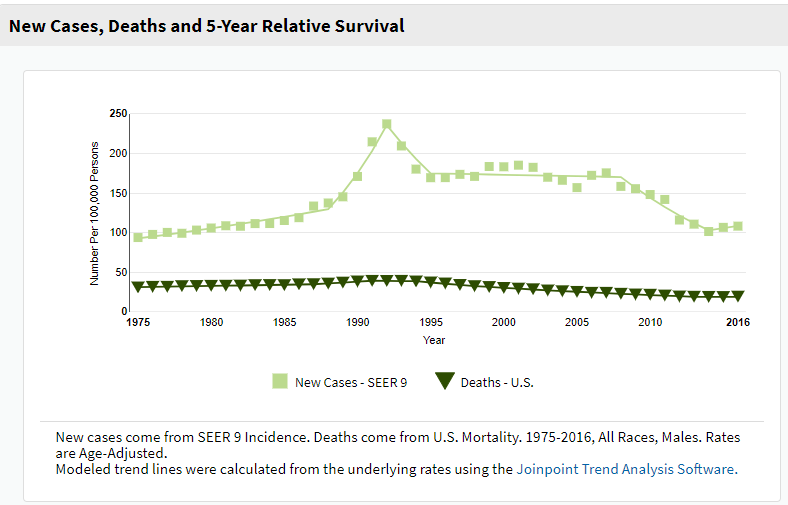
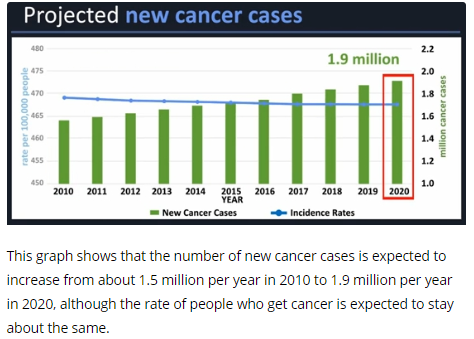
"Better-regarded sources" is weasel wording and a logical fallacy. Who's predicting this increased incidence in the U.S.? Smoking is on the downswing thus lung CA decreasing, prostate CA trends as noted above. You have previously cited one source which says the number of incident cases will increase in America by <1 million over the next 20 years and this will thus equal a ~1% rise in incidence per year. Surely you can realize that if this one single source's modeling is even mildly off... and follows the recent trend...
... incidence may flatline or decrease.*
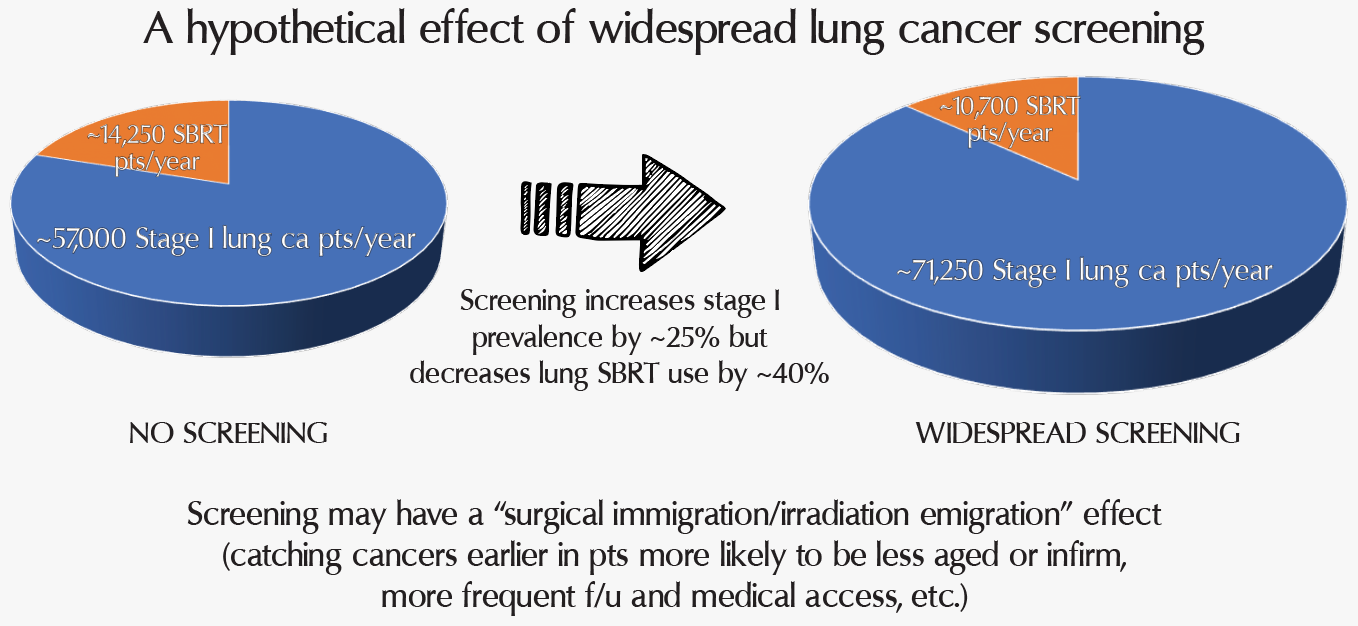
I will call you out for weasel wording again ("would agree with me"... that's nice!), and that "someone" is me. And it wasn't a claim. I was simply citing a source which revealed that at a lung nodule clinic at MGH they saw about 140 patients/year which yielded about 8 lung SBRTs a year. Draw conclusions from that as you will. But I have also cited national data showing that over a 10y period about 30,000 (out of ~150,000) patients at most got lung SBRT which translates to about 3,000 cases per year. We can be very confident that no more than ~15,000 patients per year are getting lung ca SBRT in the U.S. This number is where I get the ~3 lung SBRTs for every rad onc in America (on average) metric.
Back to your "better-regarded sources" and my "claims." Hopefully I have not made any "claims" per se. And my sources here were SEER, the CDC, The Oncologist, the JNCI, and the Red Journal. And a few random internet links for fun. However you have made claims which are, from my end, impossible to falsify. This does give you the virtue of never being provably wrong.
*even the CDC's 2015 modeling was off. They predicted ~1.9 million cases for 2020 in 2015. But now that we are five years in the future from 2015, and actually in 2020, we can better see the actual 2020 number will be about ~1.8 million for 2020. About 5% less than what the CDC predicted just 5y ago.
I believe you 100% and without any hesitation.
I also believe you are attacking a straw man.
i will respond for him: HPV cancers are also increasing because all that vaccine stuff is bunch of bull, and this will create need for more cervical brachytherapy fellowships Smoking rates are also going up so we will see increases in lung, bladder, pancreas, and heart cancers. They will all double at least to offset the doubling of residents. We will probably also treat more breast DCIS in future,
If you were going to delete anything, I think my post (even with the witty 'scarbscribe') was probably one that should go...
Always fun to go through current ASTRO job postings
Cook County Hospital / Chicago - "Where the life you save may one day take your own"
Yikes, yeah you might not be a good fit for our job. If treating lower socioeconomic and minority patients isn't your thing that's ok but most of them haven't killed me.
Maybe rad onc twitter is right - a culling of the field might get rid of this wrong type of oncologist.
There was LITERALLY a TV show called "ER" starring George Clooney based on Cook County hospital and this actually happened on the show. You may be too young to remember it, so it's where the Casamigos tequila guy-slash-social activist got famous (prior to his stint on Facts of Life). So, cool it! Sounds like you would be terribly un-fun to work with, so NO THANK YOU.
Culling people from society with no sense of humor would also be great, but in general, culling of all kinds seems .. sort of "Hunger Games" don't ya think?
Rad onc trivia: a rad onc appeared briefly one time on ER, was shown in non-flattering (lazy) light as I recall. Not quite as bad as the rad onc portrayal in The Doctor but still.There was LITERALLY a TV show called "ER" starring George Clooney based on Cook County hospital and this actually happened on the show. You may be too young to remember it, so it's where the Casamigos tequila guy-slash-social activist got famous (prior to his stint on Facts of Life). So, cool it! Sounds like you would be terribly un-fun to work with, so NO THANK YOU.
Culling people from society with no sense of humor would also be great, but in general, culling of all kinds seems .. sort of "Hunger Games" don't ya think?
Friends, I’ve stated in prior posts why I think the predictions of the future here will turn out to be wrong - I don’t have the time to address everything point by point. You can take a look back at my prior posts, and you can feel free to disagree.
Separately, I am glad someone commented on the insensitivity and unprofessionalism of the post about the different cities and patient populations represented by the job postings mentioned. I get that it may have been intended as a joke, but it strikes me as part of a common sentiment here. It’s fine if you don’t want to live somewhere, but we can’t forget that these are (collectively) our patients, and more importantly, our fellow man.
Friends, I’ve stated in prior posts why I think the predictions of the future here will turn out to be wrong - I don’t have the time to address everything point by point. You can take a look back at my prior posts, and you can feel free to disagree.
Separately, I am glad someone commented on the insensitivity and unprofessionalism of the post about the different cities and patient populations represented by the job postings mentioned. I get that it may have been intended as a joke, but it strikes me as part of a common sentiment here. It’s fine if you don’t want to live somewhere, but we can’t forget that these are (collectively) our patients, and more importantly, our fellow man.
And that's just the White House..... bazinga!We live in an era of 24 hour porn on smart phones, constant vulgarity on TV and the radio, a world where sarcasm and satire rule,
"The ABR gave a good exam and I was cyberbullied"Friends, I’ve stated in prior posts why I think the predictions of the future here will turn out to be wrong - I don’t have the time to address everything point by point. You can take a look back at my prior posts, and you can feel free to disagree.
Separately, I am glad someone commented on the insensitivity and unprofessionalism of the post about the different cities and patient populations represented by the job postings mentioned. I get that it may have been intended as a joke, but it strikes me as part of a common sentiment here. It’s fine if you don’t want to live somewhere, but we can’t forget that these are (collectively) our patients, and more importantly, our fellow man.
It’s fine if you don’t want to live somewhere, but we can’t forget that these are (collectively) our patients, and more importantly, our fellow man.
Sir/Ma'am, we are all willing to go whereever is necessary to radiate our fellow man. Unless of course there are no biryanis there. That's just inhumane.
In other news, I am deep in talks with the cafeteria staff here. The lunch lady is pretty sure she can make some killer biryanis. Time will tell, but I think there's hope...
If your interests truly lie in helping your fellow man, lets advocate docs getting out of an oversupplied specialty like radonc and entering one with shortage/need like medonc, family med, etc. There is virtually no metro under 100,000 in america that is uncovered by a linac and now with the lack of supervisory requirement, no one has to even live in small places- just fly out there one day a week!but we can’t forget that these are (collectively) our patients, and more importantly, our fellow man.
And that's just the White House..... bazinga!
Seriously though, agree with the main point.
What a bunch of sniveling weenies and shrinking violets! We live in an era of 24 hour porn on smart phones, constant vulgarity on TV and the radio, a world where sarcasm and satire rule, and if someone makes a joke about different cities and practices, that is “insensitive and unprofessional”. I know I can guarantee within 3-4 years the age group of the two people who are just so offended. What a complete farce. You are becoming caricatures of yourselves.
How did an entire generation make a culture out of getting offended?
And that's just the White House..... bazinga!
Seriously though, agree with the main point.
A truly great post. Had the most white space privilege of any post in SDN history I think.I’m pretty sure this will be deleted, but great post!
Here's the problem, @evilbooyaa
The leap goes from me making a one-off line about Cook County Hospital (notorious in the medical and entertainment community - and the line was initially associated actually with another county hospital from a reality trauma show - Charity Hospital in Louisiana) to them saying that "if treating lower SES and minority patients isn't your thing"... do you see how why those shouldn't be connected? Do you see how stating that if I make a remark about a County hospital that means I don't want to take care of the poor or minorities? It's a very odd and quite provocative thing to say and honestly, I don't think most people in my age group do that sort of thing. There is a tendency for *that* generation to basically say "if you joke about something that I care about, you are racist / anti poor / sexist / homophobic"). Which isn't really the case.
I also have a hunch that this doctor that works there is not 100% of the time talking about how great it is to work at County. If they are healthy, they probably have some coping mechanisms - i.e. "gallows humor" that they use among each other, because working at County is rough. It is challenging, the patients' stories will just kill you. If you only focus on that, and can't let go for a moment, you'll burnout quickly.
We can ascribe motives to people however we want to, call them unprofessional or insensitive, but at the end of the day, this is all signaling. No healthy physician, especially in oncology, is not engaging in some form of gallows humor as a way to get through the day. You'll note that I didn't insult individual patients, a race .. it was just a comment that Cook and the adjoining neighborhood have some crime issues.
The claim was MGH treats 8 SBRT lung patients referred specifically from their lung nodule program. I believe this was in context of an argument that lung screening will greatly increase the demand for XRT as a downstream effect.
Only if you assume that Harvard doesn’t have multidisciplinary clinic or rounds where patients are directed from nodule clinic to the correct treatment.That's still somewhat misleading as, logically, most patients who's lung cancer is found during screening should likely meet with a surgeon first anyway... right? Lobectomy is the standard of care until something like VALOR tells us otherwise. Most of my referrals for early stage lung SBRT come from surgeons for patients who are inoperable or decline surgery.
You think medical operability is always determined at thoracic tumor board? Who do you suppose orders the PFTs and determines operability?Only if you assume that Harvard doesn’t have multidisciplinary clinic or rounds where patients are directed from nodule clinic to the correct treatment.
I think that is a very poor assumption.
You think medical operability is always determined at thoracic tumor board? Who do you suppose orders the PFTs and determines operability?
I think the point is that increased lung cancer screening will do next to nothing for radonc volume. In fact, lung cancer will plummet with less smokingThat's still somewhat misleading as, logically, most patients who's lung cancer is found during screening should likely meet with a surgeon first anyway... right? Lobectomy is the standard of care until something like VALOR tells us otherwise. Most of my referrals for early stage lung SBRT come from surgeons for patients who are inoperable or decline surgery.
I think point That increased lung cancer screening will do next to nothing for radonc volume. In fact, lung cancer will plummet with less smoking
We have established ct screening program and I get about 1-2 cases a year through it. Maybe half of those 1-2 cases would have come as stage 3 if were not screened and (am loosing out on those 30 treatments) the other half I am losing out on treating brain and bone Mets.next to nothing?
are you dumb?
the more lung cancers diagnosed, the more that need treatment, some proportion of which will include radiation.
WHY ARE PEOPLE SO LOW IQ HERE
We have established ct screening program and I get about 1-2 cases a year through it. Maybe half of those 1-2 cases would have come as stage 3 if were not screened. Again mgh radonc gets 8 cases/year through their screening program?
But there will be less lung cancer diagnoses as smoking plummets. 45% 1960s to 15% today. It’s really dramatic.bottom line - if more lung cancer diagnoses are happening in the country at large, more cases will need radiation. bottom line. it really is quite simple. from a cancer business point of view, it is a good thing, just like PSA screening was back in the day. I think the jury is out on whether it is good for patients or not (no OS benefit or overall cancer mortality benefit)

Ummm, yes. I’ve worked in community hospitals where CT surgeons, pulmos, and rad oncs review nodules/patients and coordinate treatment. I’m guessing Harvard may be (has been) able to pull this off.You think medical operability is always determined at thoracic tumor board? Who do you suppose orders the PFTs and determines operability?
Here is a graph of smoking incidence: \next to nothing?
are you dumb?
the more lung cancers diagnosed, the more that need treatment, some proportion of which will include radiation.
WHY ARE PEOPLE SO LOW IQ HERE
Could be less than nothing, not next to nothing. Further elaborated, IQ-controversial version.next to nothing?
are you dumb?
the more lung cancers diagnosed, the more that need treatment, some proportion of which will include radiation.
WHY ARE PEOPLE SO LOW IQ HERE
Could be less than nothing, not next to nothing. Further elaborated, IQ-controversial version.
1. JK Jang, JC Ye, SM Atay, et al. Temporal Trends in the Utilization of Stereotactic Body Radiotherapy for Non-Small Cell Lung Cancer in the United States. IJROBP 2019;105:E511.
2. Roberts TJ, Lennes IT, Hawari S, et al. Integrated, Multidisciplinary Management of Pulmonary Nodules Can Streamline Care and Improve Adherence toRecommendations. The Oncologist 2019;24:1-7.
3. Stage at Diagnosis | Cancer Trends Progress Report
It is very possible my IQ is less than residents following me from more competitive years, so this should be pretty obvious!Could be less than nothing, not next to nothing. Further elaborated, IQ-controversial version.
1. JK Jang, JC Ye, SM Atay, et al. Temporal Trends in the Utilization of Stereotactic Body Radiotherapy for Non-Small Cell Lung Cancer in the United States. IJROBP 2019;105:E511.
2. Roberts TJ, Lennes IT, Hawari S, et al. Integrated, Multidisciplinary Management of Pulmonary Nodules Can Streamline Care and Improve Adherence toRecommendations. The Oncologist 2019;24:1-7.
3. Stage at Diagnosis | Cancer Trends Progress Report
Smoking plummeting by 2/3 is a liberal assumption and that this will impact lung cancer incidence is a liberal assumption?This liberal use of assumptions and hand waving with numbers shtick has really run its course - but like Trump, it gets you likes from the ‘little people’ as Evil calls them - so you do you!
Smoking plummeting by 2/3 is a liberal assumption and that this will impact lung cancer incidence is a liberal assumption?
Pretest probability significantly impacts future effects on radiation utilization related to screening.We are talking about lung screening effect (and scarb’s Nonsense) not the smoking use decline, which will decrease a number of cancer diagnoses hopefullly.
Lung screening effect is obvious.
It will convert stage III/IV cancers to stage I/II cancers. This is literally the reason why screening(of any sort) exists.
We treat the vast majority of stage III/IV lung cancers with 10-35 fractions of radiation. Often multiple times.
We DON’T treat the vast majority of stage I/II lung cancers. When we do, it’s usually once for 3-5 fractions.
I know I’m dumb, and making controversial assumptions, But lung screening should be seen as a great thing for our patients and a net loss for rad onc work.