- Joined
- Jan 20, 2013
- Messages
- 1,945
- Reaction score
- 645
Click through each section to learn more about the case and refine your differential diagnosis.
A 33-year-old man with no significant past medical history presented to the emergency department with chest pain. The pain began 2 days ago, is described as pleuritic and is moderate in severity (5-6 out of 10), is substernal, and is worse with exertion. He adds that he’s also been experiencing a week of non-bloody loose stools, 5-6 times per day, which resolved yesterday.
Your Assessment
Which of the following is the most likely diagnosis?
A. Myocardial infarction
B. Pulmonary Embolism
C. Aortic Dissection
D. Pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
Global Morning Report (GMR) is a daily series of fun, interactive, and brief clinical cases for physicians and trainees to practice their clinical reasoning in just a few minutes each day. GMR is a medical education initiative from the Human Diagnosis Project.
Solve more cases like this during GMR’s 'Chest Pain Challenge' the week of February 18th! Each case will feature a chief complaint of chest pain.
A 33-year-old man with no significant past medical history presented to the emergency department with chest pain. The pain began 2 days ago, is described as pleuritic and is moderate in severity (5-6 out of 10), is substernal, and is worse with exertion. He adds that he’s also been experiencing a week of non-bloody loose stools, 5-6 times per day, which resolved yesterday.
Your Assessment
Which of the following is the most likely diagnosis?
A. Myocardial infarction
B. Pulmonary Embolism
C. Aortic Dissection
D. Pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
Your physical exam reveals the following:
Which of the following is the most likely diagnosis?
A. Myocardial infarction
B. Pulmonary embolism
C. Aortic dissection
D. Acute pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
- Vital signs: Within normal limits.
- Cardiovascular exam: Regular rate and rhythm, normal S1 and S2, no murmurs, rubs or gallops and no jugular venous distention.
- Lung exam: Clear to auscultation bilaterally, no wheezes, no rales, and no rhonchi.
- Abdominal Exam: Soft, non-tender, non-distended, normal bowel sounds.
- Musculoskeletal: No pain to palpation of rib cage.
Which of the following is the most likely diagnosis?
A. Myocardial infarction
B. Pulmonary embolism
C. Aortic dissection
D. Acute pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
A laboratory and radiographic evaluation is significant for:
Troponin: On presentation 1.5 ng/mL (positive); 6 hours later: 0.9 ng/mL (positive)
Complete blood count and basic metabolic panel are unremarkable.
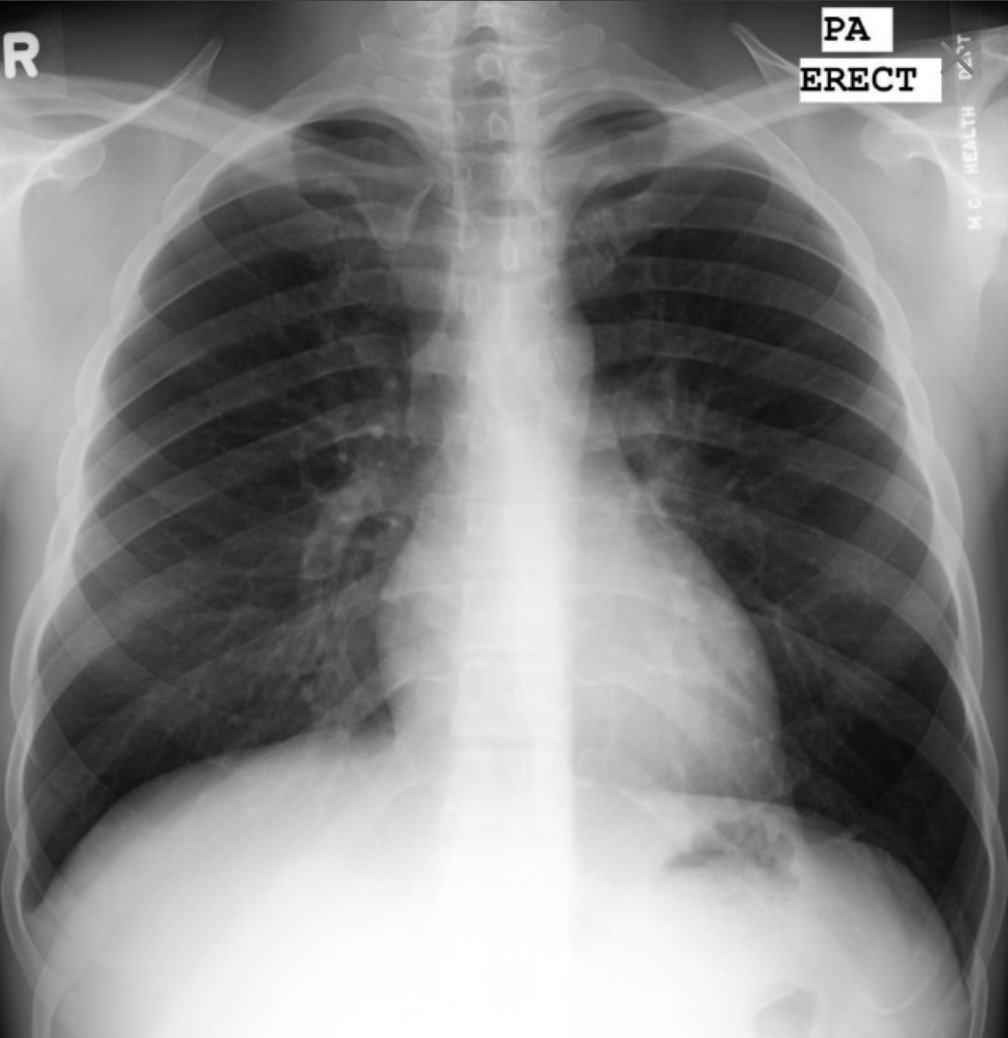
CXR revealed:
Your Assessment
Which of the following is the most likely diagnosis?
A. Myocardial infarction
B. Pulmonary embolism
C. Aortic dissection
D. Acute pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
Troponin: On presentation 1.5 ng/mL (positive); 6 hours later: 0.9 ng/mL (positive)
Complete blood count and basic metabolic panel are unremarkable.
CXR revealed:
Your Assessment
Which of the following is the most likely diagnosis?
A. Myocardial infarction
B. Pulmonary embolism
C. Aortic dissection
D. Acute pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
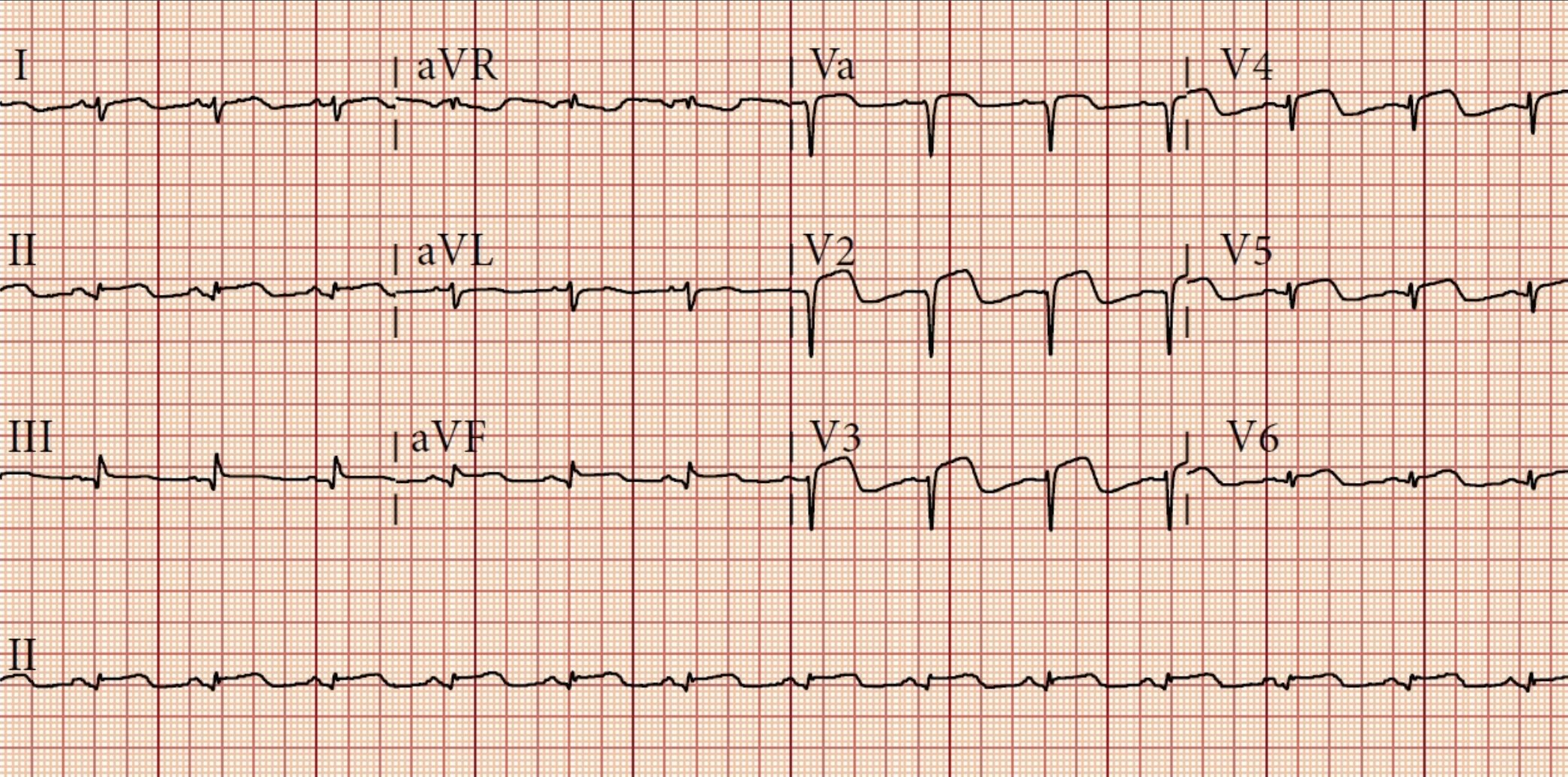
EKG revealed:
Echocardiogram showed:
LV ejection fraction and wall motion: Normal
Valves: Normal
Pericardial effusion: Trace
Your Final Assessment
A. Myocardial infarction
B. Pulmonary embolism
C. Aortic dissection
D. Acute pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
Echocardiogram showed:
LV ejection fraction and wall motion: Normal
Valves: Normal
Pericardial effusion: Trace
Your Final Assessment
A. Myocardial infarction
B. Pulmonary embolism
C. Aortic dissection
D. Acute pericarditis
E. Gastroesophageal reflux
F. Esophageal tear
The Human Dx medical community concluded answer D: Pericarditis. Solve more cases by signing up for Human Dx here.
Teaching Points:
Teaching Points:
- Case Resolution: The patient's chest pain resolved within three days of initiation of NSAIDs/colchicine and did not recur. Subsequent ECGs showed resolution of ST elevations and persistence of T wave inversions. The chest X-ray was read as normal. Exercise stress testing was normal.
- Diagnosis: The diagnosis of acute pericarditis requires at least 2 of 4 criteria: pericardial friction rub on exam, chest pain, typical ECG changes (widespread ST elevation with T wave inversion in this patient), or pericardial effusion on echocardiography. In the absence of other plausible explanations for his elevated troponin, two of these four criteria is sufficient to make a diagnosis in this patient.
- Etiology: The cause of 80-90% of pericarditis are unknown but thought to be likely viral in nature. Many patients have evidence of a recent viral infection (diarrhea in this patient).
- Treatment: The mainstay of treatment are nonsteroidal antiinflammatory drugs (NSAIDS) and colchicine. Colchicine has been shown to minimize risk of recurrence.
- References: Reference: LeWinter MM. Clinical practice. Acute pericarditis. The New England journal of medicine 2014;371:2410-6.
Global Morning Report (GMR) is a daily series of fun, interactive, and brief clinical cases for physicians and trainees to practice their clinical reasoning in just a few minutes each day. GMR is a medical education initiative from the Human Diagnosis Project.
Solve more cases like this during GMR’s 'Chest Pain Challenge' the week of February 18th! Each case will feature a chief complaint of chest pain.