- Joined
- Jan 19, 2011
- Messages
- 216
- Reaction score
- 69
- Points
- 4,751
- Attending Physician

We always did routine alines for Afib ablations under general. not so much for aflutter/svt ablations. My current gig rarely does them at all in EP. what is your practice?
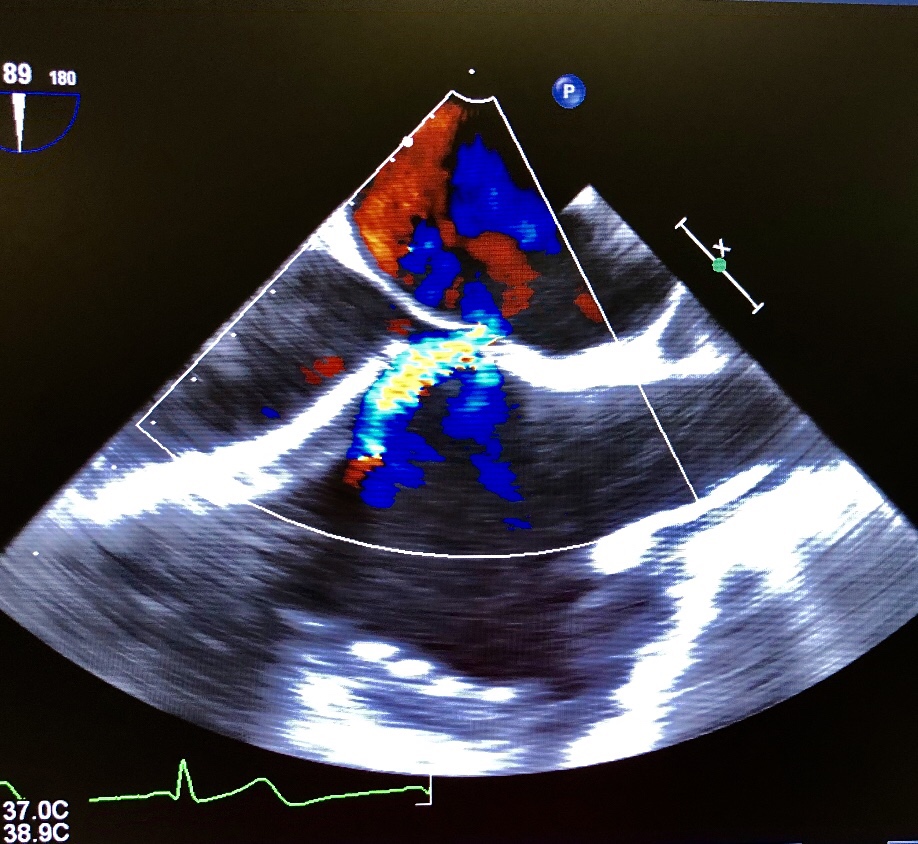
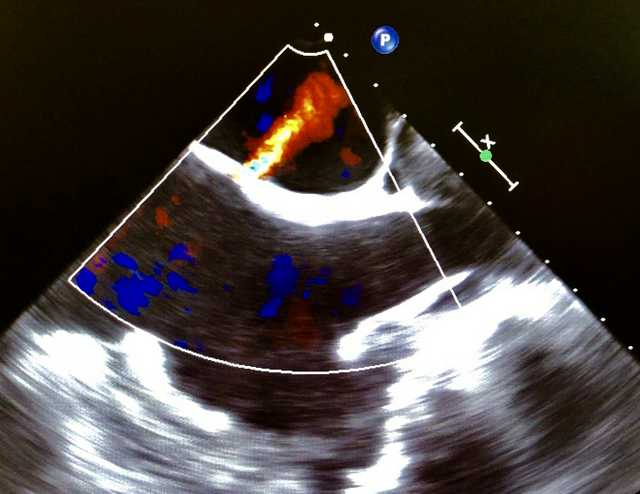
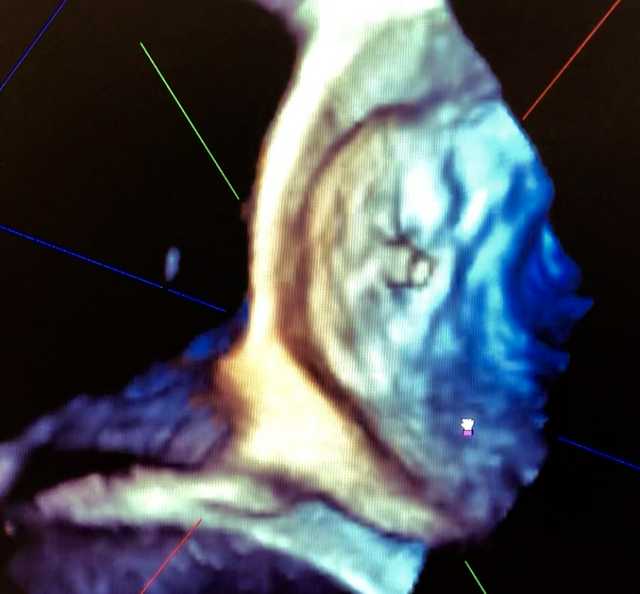
We had one a couple weeks ago.Certainly have had my fair share of iatrogenic effusions/tamponade in the Cath lab.
Certainly have had my fair share of iatrogenic effusions/tamponade in the Cath lab.
Never done one for an Afib ablation.
Interesting to see such a difference in practice; that doesn't occur for too many procedures in anesthesia.
i guess it depends on how good the proceduralists are at different places.
You ever done an afib ablation with a patient who has PA systolics in the 90-130 range? What would you worry about?
No a line for a fib ablations here unless very sick.
No, never done them on sick patients: they all seem to be middle age over weight with aceptable cardiac function.You ever done an afib ablation with a patient who has PA systolics in the 90-130 range? What would you worry about?
No, never done them on sick patients: they all seem to be middle age over weight with aceptable cardiac function.
Academic center, very slow fellows/attendings with almost all get pre induction aline as requested by cardiologist and they still place a femoral sometimes.
Awake art lines for ablations? What’s the cardiologist reasoning for this?
Lot of them have crap hearts and get hypotensive quick on induction even if you're careful. There is also a distinct possibility of crashing right there on the table, away from the main ORs.