Bariatric surgery only boomed when it got approved by Medicare that was. In mid 2000s.
Than private insurers started approved more. And obviously advances in surgery especially with gastric sleeve becoming more and more popular where it dominant type of weight loss surgery over the original gastric bypass.
I would never use the word “always” though
like open heart and valve surgeries were booming up to the early 2000s. Than it went down even with patient population grew. Because cardiologist started doing more invasive procedures that drove down many open heart procedures. Now most cv surgeons are hospital employed because revenue stream is so uneven. Before most were private.
With fda just now approving weight loss wegovy for cholesterol control this week. This likely will blow up the door to force private insurers to cover those drugs. Those drugs will likely become the standard weight loss vs invasive surgeries. There are non fda. Approved GI procedures that my friend had in Mexico.
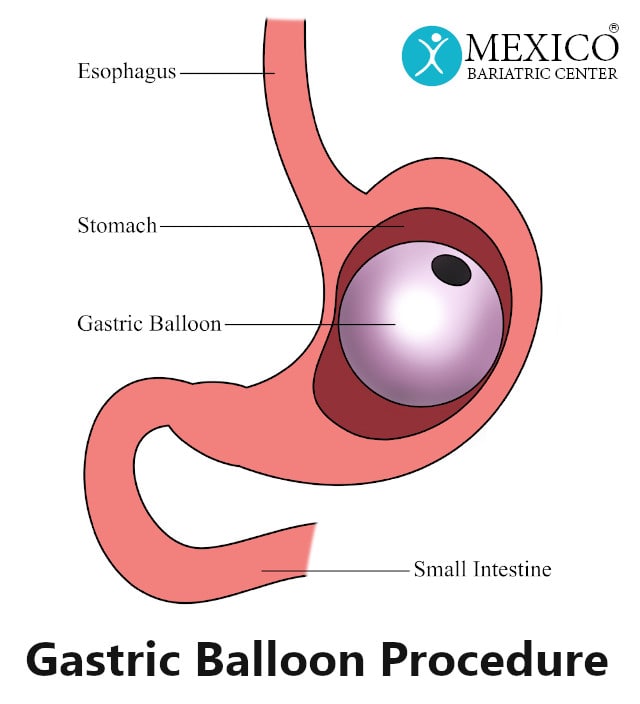
In the Gastric Balloon procedure, a balloon is inflated in the stomach to temporarily decrease the stomach capacity/volume and induce weight loss. The goal of this procedure is to be somewhere in between major weight loss surgery and dieting/exercise. The gastric balloon works best with a...

mexicobariatriccenter.com
It’s very effective. She lost 50 pounds in 9 months. Flew back to get it removed. On ozempic and lost another 40 pounds. So she went from 215 down to 125 without invasive gastric sleeve which most have been doing