- Joined
- Feb 13, 2008
- Messages
- 545
- Reaction score
- 9
That doesnt make any sense. It is way too much effort and sacrifice to take such long training for no more $$. Are you saying that having more training and knowledge is pointless then? You think that a FM person should get paid the same as an orthopedic surgeon, a neurosurgeon, rad onc, etc? Why don't we all work for nurse wages too then?
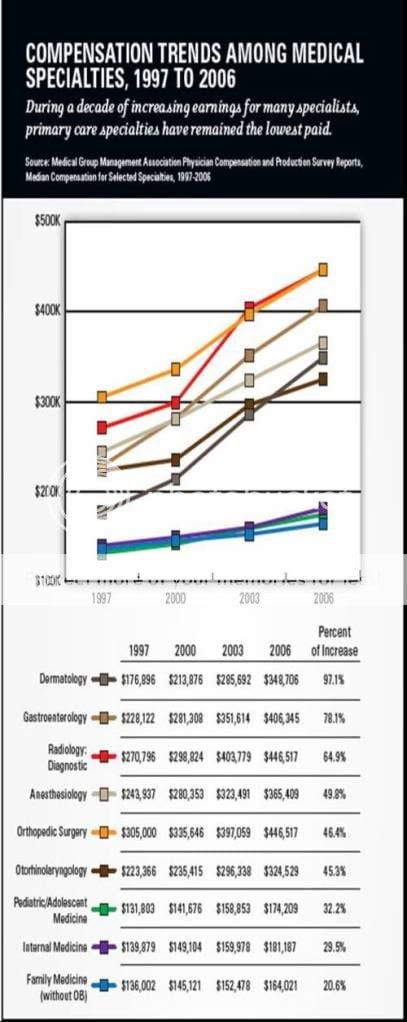
200k is roughly what you guys make. Radiologists train double the time you guys train. why should they not get paid more? They have more knowledge, skills, and realistically add much more to patient care. Not to start a flame war, but 90% of primary care can be done by a midlevel.
Again explain to me why all specialties would get paid the same? Then nurses should make the same we do then, as well as techs, janitors, etc.
Your statements are really dense. As a hospitalist and generalist I have much broader knowledge than specialist physicians although I make it a point to learn from them whatever they have to offer. You can not seriously be stating that internal medicine, family medicine and pediatrics represent small knowledge bases That can be mastered without yrs of dedication and training when they are in fact extremely broad and serve as the foundation of all other specialties. Cost savings is achieved by physicians with broad enough knowledge to not have to consult and thats what things are moving towards. We don't get "stuck" very often. Consults most often are for procedures ie Cath's, scopes, surgeries, ivc filters, or legal cover or just patient demand at times rather than fighting the patient. Also, I have seen piss poor cardiology coming from "cardiology" midlevels and piss poor "critical care" from critcal care mid levels. While the big boss ie Dr. Is doing Cath's all day (because that's where the money is) all too often to the point where sometimes you wonder if you are doing the patient a disservice rather than a favor by consulting cards in the first place with the only real benefit being legal cover. To those that would say hospitalist medicine isn't primary care I would say that it's nothing more than an extension of out patient medicine and the skill of the outpatient physician determines what can be managed outpatient vs inpatient again pointing to cost savings by competent primary care physicians not mid level hacks or a specialist who needs to consult 5 other specialists to do the job of one primary physician.
Last edited: