Discussing possible changes to the match or residency applications is good. There's often a thread about it this time each year. A prior thread is here:
NRMP Match: Good, bad or ugly? | Student Doctor Network
Currently, after match / SOAP / scramble, essentially 100% of all spots are filled. So any change to the match or application system isn't going to improve position fill rate -- benefits would be decreasing cost of applications, and distribution of positions (i.e. whom gets what spot). Decreasing costs is always a good goal. Anytime someone gets a spot that they are happier with, it's quite possible that someone else will get something they are less happy with, measuring how happy people are with the match is complicated.
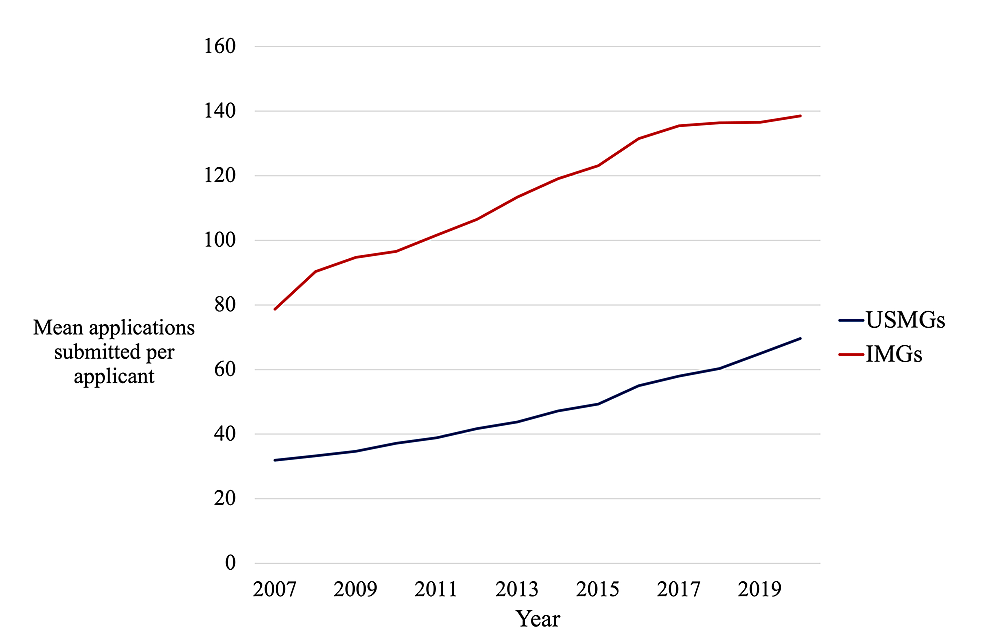
Proposals to changing the app process include an application cap and signaling (via Gold/Silver/Bronze application limits, or some other mechanism). Getting ERAS to decrease fees for apps is also often discussed, but unclear how that could happen as neither PD's nor students have any leverage -- honestly starting a new application service to compete with them would be the most effective. App caps or signaling are a mixed bag -- each application may have more chance of being fully reviewed, but applicants would need to choose carefully where they want to send their applications, and some programs have benefitted from app inflation. App caps are specifically problematic for couples and for anyone with a "red flag" -- and I doubt we would all agree on what that constitutes.
Proposals to changing the match include an early round for all, a two phase match with the first round for US grads (or US citizens) only. Some suggest doing away with the match entirely. If the early round was complete before the main application phase, that would cut down on applications.
Programs being required to publish their criteria is theoretically reasonable, but unclear how feasible it really is. Let's say I publish that my step cutoffs are 210 and 230. What happens with people who have a 206 on S1 and a 278 on S2? We might require different criteria for DO's and IMG's at some programs, and the criteria might even be school related (i.e. programs might use different criteria for students from schools they have no experience with). And isn't the point of all of this to get away from criteria and move to holistic review?