I mean we shouldn’t all shut up. It’s just my take is the future is the worry, and the present is mostly still okay, when it comes to the market.
I generally agree, but I also agree that the interest in radonc by med students is right now about what it should be. I strongly disagree with maintaining resident complements at current levels.
IMO, the market today is OK by the following standards:
1. You can get a job
2. You cannot with high confidence determine where you are going to get a job
3. The type of job you get is likely to be incommensurate with your credentials (may change as credentials of applicants decrease)
4. Your lateral mobility will be close to zero
How do I know this? Because I've hired someone in the past several years. All national applicants for a job that was a regional job for me and that I thought I was too good for years ago. Every applicant we interviewed had multiple real publications and some affiliation (either undergrad, medical school, residency or faculty) with one of the most prestigious institutions on earth (IVY or Big 3 type cancer center). It was easy to hire someone excellent at a cancer center where all medical oncologists are IMGs.
It's completely silly to denigrate people who do fellowships to enhance their academic credentials or do meaningful research. Now I admit, when my chair recommended that my 38 year old, children having, PhD having self "consider a fellowship" if I wanted to "do something serious" I was appalled and realized that my academic career was over. However, the "most serious" people have always been willing to do this sort of thing, even go back to residency and get double boarded. They have always been willing to do a national job search. Like most community docs, I have come to terms that within my field, I am not "serious". I do believe that this dichotomy is less severe in many other fields.
As I've said before, radonc will remain for the foreseeable future an option that provides low intensity clinical practice with above average academic pay for "truly, truly elite" research types. We are talking the Tim Chans and Max Diehns of the world. (Who of course could do whatever they wanted in any field
and study whatever they want now).
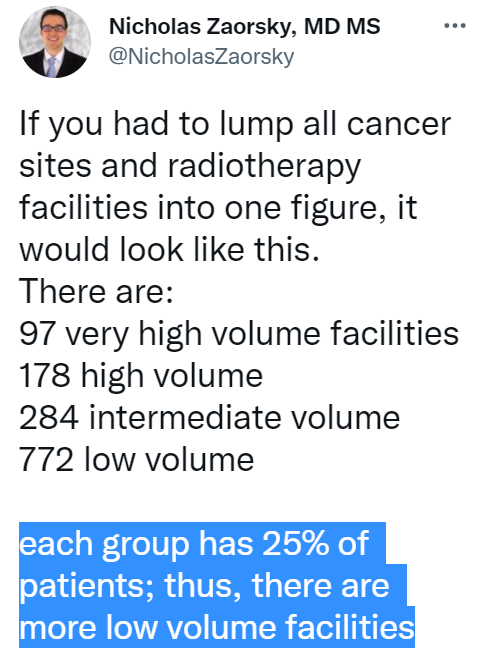
I am skeptical of the details of Wallnerus' data. (not his analysis or integrity). The main issue I have is that the total number of "working" radoncs is not well defined. Heck, there are docs that show up on regional "top docs" lists that haven't practiced in years. When you go to part time or essentially retire, nobody takes your license away.