- Joined
- Jan 13, 2015
- Messages
- 4,931
- Reaction score
- 6,856
Bunny Ranch.....wait, what was the question?😎I would give anesthesia for free if I got to live in the Playboy mansion. That's my idea of a desirable place.

Bunny Ranch.....wait, what was the question?😎I would give anesthesia for free if I got to live in the Playboy mansion. That's my idea of a desirable place.
What's the alternative? One can choose to live rather humbly and work for an AMC or try for the gold at the end of the rainbow. The difference between the income of an AMC vs 95th percentile MGMA is almost double per year. Over a 25-30 year career this is worth multiple millions more in savings to those willing to put in the 5 years.
Do I think the current system of billing $120 per unit is going to persist? No. I think 3-4 years after Biden/Harris wins the White House the shift in healthcare will be very obvious. Obama passed the ACA and Biden along with the Democrat Senate in 2021 are going to pass more revisions to the ACA allowing a public option along with an early medicare option (for those 60 years and older). This will mark another shift away from private insurance carriers towards government single payer healthcare.
But, I think the current system has at least 8-10 years left in it before undergoing radical change towards a complete single payer system. I do think that will happen in my lifetime but it is going to take another much more progressive administration to push for and pass a 100% single payer system. That could be Harris or AOC down the road.
I will concede that I should have gone to the NBA, however. I think I needed about 5 more inches and a stronger work ethic in HS.
Yes. Like nyc and getting paid minimum wage.... I totally understand. But this was not nyc. This was more for the promise land, of mgma 95%.... in five years if you’re lucky, 7 if you aren’t.
The problem is that the promised land may not exist in 5-7 years. Even for those who currently reside there.
The problem is that the promised land may not exist in 5-7 years. Even for those who currently reside there.
Because the other non-uber competitive specialties suck for a variety of reasons compared to even the worst case anesthesiology scenario.
the problem with the future isn't with anesthesia, it's with medicine in general
Honestly, this thread could've been closed after the first two replies:
Still the best place to practice medicine, still no state income tax, still a nice place to live.I like reading the threads from 10 years ago about how Texas is such a great place to practice, no state income tax, nice place to live and now they are all owned by AMCs.
That'd be a funny statement if it wasn't so sadly inaccurate.Most of the cost-cutting will be on the administrative side due to the complex and bloated insurance billing infrastructure, not reimbursement.
I would encourage you to ask real life anesthesiologists. SDN tends to be very pessimistic. Our residents/fellows have had no issues finding good jobs.MS4 seriously thinking of applying to anesthesia instead of ortho. Is the field really dead/dying? The job market seems pretty good right now
That'd be a funny statement if it wasn't so sadly inaccurate.
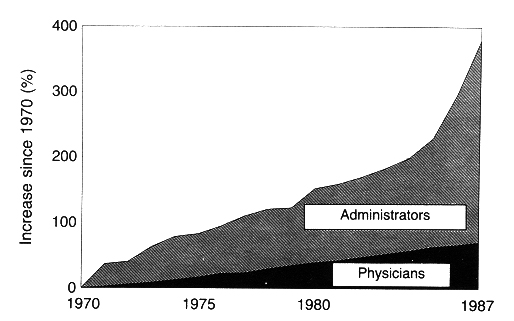
That chart ends in 1987 when things had already spiraled out of control. I only include it to illustrate that this is an old, old problem that hasn't been solved because the people making the "solution" are pulling fat paychecks in that gray blob of the chart.
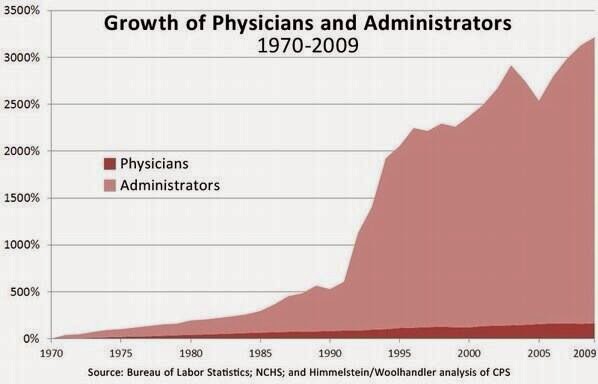
Here's a more current chart:
But I totally believe 2021 is the year we reverse 50 years of administrative bloat. Totally.
Healthcare reform will be another handout to insurance companies, pharmaceutical companies, device companies, with another layer of administrators in between.
This is exactly why insurance companies will lobby like hell to make sure that whatever gets passed will (at the very least) not make them extinctLets use common sense. If M4A is passed, everyone is covered under medicare/medicaid. There will not be any insurance companies (unless Congress pushes for a public option instead of M4A). If there are no insurance companies, there will not need to be as many administrators doing the pre-auths, billing, coding, etc... There would be no real reason large institutions would keep unnecessary bloat, if its eating into their balance sheet. Lastly, chart discusses the growth of administrator positions, not compensation of those administrators, so your comment about "people making the "solution" are pulling fat paychecks in that gray blob of the chart" is silly at best. Most executive compensation is tied to milestones, one of which is their net profitability; hence, less reason to keep administrative positions that serve less of a purpose in a healthcare system that does not have a dominant private insurer base.
Applying to a different specialty but it just doesnt make sesne that M4A would get passed. How will companies with trillions behind them simply dissappear when they have tremendous lobbying power? Highly doubt it will happen.Lets use common sense. If M4A is passed, everyone is covered under medicare/medicaid. There will not be any insurance companies (unless Congress pushes for a public option instead of M4A). If there are no insurance companies, there will not need to be as many administrators doing the pre-auths, billing, coding, etc... There would be no real reason large institutions would keep unnecessary bloat, if its eating into their balance sheet. Lastly, chart discusses the growth of administrator positions, not compensation of those administrators, so your comment about "people making the "solution" are pulling fat paychecks in that gray blob of the chart" is silly at best. Most executive compensation is tied to milestones, one of which is their net profitability; hence, less reason to keep administrative positions that serve less of a purpose in a healthcare system that does not have a dominant private insurer base.
Agreed. However, my initial post was in response to blade's assumption on what would happen if it were to pass, not on the likelihood of it passing.Applying to a different specialty but it just doesnt make sesne that M4A would get passed. How will companies with trillions behind them simply dissappear when they have tremendous lobbying power? Highly doubt it will happen.
I dunno while porn looks fun, per se, you get paid more in the NBA and if you’re good enough end up sleeping with the same people.....in a non-bubble world of course 😎Many could say the same about a career in pornography
Honestly these two fields are so different it really just depends on what you want to do. Both have their issues, but do you want to be the Quarterback or the offensive left tackle? Both are very important to the offense and both are paid well but one is treated much different than the other.MS4 seriously thinking of applying to anesthesia instead of ortho. Is the field really dead/dying? The job market seems pretty good right now
Honestly these two fields are so different it really just depends on what you want to do. Both have their issues, but do you want to be the Quarterback or the offensive left tackle? Both are very important to the offense and both are paid well but one is treated much different than the other.
keeping it 100.....you can’t go wrong with either choice it’s just you day to day and lifestyle will be different......and one has OB call
I think you're catching my drift. 🙂Lets use common sense. If M4A is passed, everyone is covered under medicare/medicaid. There will not be any insurance companies (unless Congress pushes for a public option instead of M4A).
Agreed. However, my initial post was in response to blade's assumption on what would happen if it were to pass, not on the likelihood of it passing.

 www.motherjones.com
www.motherjones.com
I am not predicting M4A this election cycle. What I am predicting is that the individual mandate is brought back (passed) and maybe Biden can get through a Medicare buy-in for those 60 years or older. Also, I predict a law which prevents OON surprise medical billing.
I do think we end up with a single payer system where the private sector is also involved in selling "enhanced advantage" plans to those that can afford it.
Everyone gets basic care of some sort like VA, Tricare, Medicare or Medicaid with the option of buying into these enhanced plans. The healthcare lobby is so strong I don't think they will just disappear in 10 years but will evolve with the social healthcare system. Plus, the U.S. will be dead broke in 10 years with a national Debt so high that only a fool would think the U.S. could afford Gold level healthcare for all its citizens. Instead, the Dems will sell basic, Iron level healthcare as though it was Gold plated to the public while those with money will purchase premium enhanced advantage plans.
This is the way most of the other first world nations provide healthcare for all its citizens. Healthcare should be provided for all people in a nation but that level of healthcare differs greatly in many European countries. As expected, those with money purchase premium plans or additional private insurance to gain access to premium level service/private hospitals and the best care possible.
Can someone explain to me how decreasing Medicare eligibility age to 60 saves money? Wouldn’t this essentially be medicare taking over the oldest most expensive cohort from private insurance? Private insurance funds itself with premiums. Who funds Medicare?
Decreasing medicare age to 60 kind of seems like boomers pulling a fast one on the younger generation so the wealthier ones can retire earlier. Reminds me of the health insurance mandate requiring young healthy people in their 20s who don’t use or need health care services to pay into the premium pool to again fund the older generation. It’s frustrating paying into broken systems that seem unlikely to be around by the time we would actually see any benefit.
Well, buying into Medicare at age 60 vs paying for your own private insurance (husband and wife) is probably worth $10-$15K per year in savings to the couple. I agree the taxpayer doesn't save a dime. I assume Biden just wants to gradually pull more people into Medicare so he can claim a small victory for his base. Maybe, it is age 60 in 2021 and age 50 in 2025? Many Progressives think this is a process which takes a decade or more in order to phase into a single payer system.
I’d still do anesthesiology if I were a MS4, but I would maybe have chosen a different (ie cheaper) place to practice.
That’s true. For me personally it’s a “better the devil you know than the devil you don’t” situation I wrestle with. The job isn’t great but it’s come to a point where I know everyone and everyone knows me. Pushing “reset” on all of this is tough but I do understand that all reward players involves some bit of risk. At some point I’ll just have to “man up”Never too late to make that change.
That’s true. For me personally it’s a “better the devil you know than the devil you don’t” situation I wrestle with. The job isn’t great but it’s come to a point where I know everyone and everyone knows me. Pushing “reset” on all of this is tough but I do understand that all reward players involves some bit of risk. At some point I’ll just have to “man up”
Most Long term partnership tracks today:View attachment 317851