- Joined
- Jul 5, 2020
- Messages
- 4,422
- Reaction score
- 9,565
- Points
- 4,861
- Attending Physician
md only

Right.md only
Sadly in most states, the opposite is the strategy. Typically CAA legislation is used as a pawn or threat in order to stave off a CRNA independent practice bill. It kind of reaches a point of trench warfare stalemate where the state Anesthesiologists don't aggressively push for an AA bill and the NAs don't aggressively push for an independent practice bill. In the end, physicians will be the suckers left holding the bag because the NAs aren't going to just sit back and not push for independent practice. It'll happen eventually, and if it happens in your state, wouldn't you want to be able to have the option to hire AAs instead? Unfortunately, in my experience, many states are going to be caught off guard when CRNA independent practice passes in their state and they didn't preemptively try to get AAs in--now there's no threat for the CRNAs and they can fully mobilize against a reactionary AA bill.
I agree with the overall sentiment, but just as a contrast, I already practice in a CRNA independent state without AAs. ACT is the predominant model here and there’s no decline in sight. There are CRNA-only hospitals in rural locations but that’s likely (hopefully) driven by the reimbursement scheme of rural pass through. The big AMCs have lost contracts and have almost no foothold. AAs would be great, however, at this point, it seems modifying the rural pass through would be the thing that really determines how likely it is for anesthesiologists to expand their presence in the state.
WI, OTOH, IS an AA state, and are losing hospitals to CRNAs with a fireman MD.
This issue is really state by state, but I agree that AAs should simply be legal across the country rather than a state decision. It’s weird to have an entire profession unable to practice in one state, but then freely in another. Off the top of my head I can’t think of many other professions like that.
All professions are regulated at the state level, it's just that AAs have only been around since the late 60's, and didn't expand much outside of OH and GA until the 2000's. By then, the CRNA lobby had gotten very strong, and they've put up incredible resistance in each state where AA legislation is proposed.
In states like the one where you live, with CRNA independent practice or even with just CMS opt out, I don't know why the state components of the ASA don't go full force for passing AA legislation. Well, I do know, and the answer is there are a lot of cowardly physicians that are content with the status quo. Very few to no one willing to stick their neck out there and protect the profession if it means rocking the boat in their local group.
It needs to come from the society without identifying individuals and would be nice if it was an anonymous vote within the society that forces the hands of the leadership to pursue AA legislation. It’s a big ask to risk losing a job or uprooting family for a potentially crappier job because you are the upsetter of apple carts. You aren’t just sacrificing yourself, but potentially your whole family. As an early career doc, that’s not being selfish or cowardly. Its instead a risk-benefit calculation tilted toward protecting family.
CRNA bullies. "If you hire an AA, the entire CRNA group will leave."I understand that perspective, I just think the threats made to people supporting AA hiring or AA legislation are almost always completely empty. No reasonably sized group has had a mass exodus of CRNAs because of reaction to AA support despite their threats. They just use those threats to control the physicians in their groups to do their bidding. Also there’s no reason why a physician can’t support AA practice and also still support the clinical staff in their group. Everyone seems to make it into an either or/all or none situation.
Yeah, All MD conversion to ACT with only AAs has been done across the country and has been very successful. The physicians love a high performing team where members of the team aren’t colluding to betray you and replace you.CRNA bullies. "If you hire an AA, the entire CRNA group will leave."
This is why the people who need to spearhead this are ones in physician only groups who do not have CRNAs to have walk out.
Start an AA program at an Physician solo group.
Wow!... It takes a strong AA to stand up to the bully CRNAsI was one of two AAs that started 10 years ago in a group of 30 MD/70 CRNA. The threats came, the docs called their bluff, and no one left. That group is now 50% AA 50% CRNA and everyone gets along well.

 www.eakc.net
www.eakc.net
That’s what they said when we brought in our first AA in my old group.CRNA bullies. "If you hire an AA, the entire CRNA group will leave."
This is why the people who need to spearhead this are ones in physician only groups who do not have CRNAs to have walk out.
Start an AA program at an Physician solo group.
howd you react to that?That’s what they said when we brought in our first AA in my old group.
Guess how many left?
They refused to speak to the AAs, wouldn’t eat lunch with them, and tried to strong arm us and refuse to give them breaks(that didn’t go well for them), but nobody left. They stayed and acted like a bunch of middle schoolers.
That’s what they said when we brought in our first AA in my old group.
Guess how many left?
They refused to speak to the AAs, wouldn’t eat lunch with them, and tried to strong arm us and refuse to give them breaks(that didn’t go well for them), but nobody left. They stayed and acted like a bunch of middle schoolers.
No - but same problem - rarely is anyone willing to call the bluff.Is it legal for those crnas to make a threat like that?
Sent them home for insubordination, and they didn’t get paid for the rest of that day. Official write ups were done. We never ran super lean, so we pulled docs to finish cases and increased supervision ratios. Some docs had to work post call. We knew this would be temporary one way or another.howd you react to that?
No - but same problem - rarely is anyone willing to call the bluff.
I don’t know honestly. Didn’t matter to us because we had a 3 strikes and you’re out policy and they were written up every time they refused. So they would’ve been gone quickly if they had continued.Is it legal for those crnas to make a threat like that?
Sent them home for insubordination, and they didn’t get paid for the rest of that day. Official write ups were done. We never ran super lean, so we pulled docs to finish cases and increased supervision ratios. Some docs had to work post call. We knew this would be temporary one way or another.
After several of them missed half their normal hours and realized we weren’t giving in they stopped.
People usually act right when their livelihood is affected.
Well I suppose we had the luxury of not really needing them. Our state allowed AAs, we had enough staff to run rooms without the troublemakers, and we had a pool to hire from if we needed new folks.Strong work!!
My idol!! Mr. No Messing Around!!! Love it. Glad you and your partners stuck to your guns. We need more like you around. Strong work!!Sent them home for insubordination, and they didn’t get paid for the rest of that day. Official write ups were done. We never ran super lean, so we pulled docs to finish cases and increased supervision ratios. Some docs had to work post call. We knew this would be temporary one way or another.
After several of them missed half their normal hours and realized we weren’t giving in they stopped.
People usually act right when their livelihood is affected.
And how do they get along these days?I don’t know honestly. Didn’t matter to us because we had a 3 strikes and you’re out policy and they were written up every time they refused. So they would’ve been gone quickly if they had continued.
We need to reduce our dependence on CRNAs, when they lose their leverage groups don’t need to cow tow to the mob like behavior we see all too often. I have never seen that behavior from AAs, and I’ve worked with tons of them.My idol!! Mr. No Messing Around!!! Love it. Glad you and your partners stuck to your guns. We need more like you around. Strong work!!
I am not sure, last I heard the group was thriving and preferentially hiring AAs. They were about 50/50 CRNAs and AAs the last time I checked.And how do they get along these days?
Posted this in another thread but meant to post it here.
Darwin’s Law of Natural Selection: Eliminating Medical Direction Anesthesia Delivery Models. » Excel Anesthesia
By Jean Covillo, DNAP, MA, CRNA Any healthcare facility that employs Anesthesia Assistants is trapped into using ONLY the costly medical direction model! Currently, there are approximately 54 million Medicare enrollees, but by 2030, this will rise to nearly 80 million.1 Medicare reimbursement...
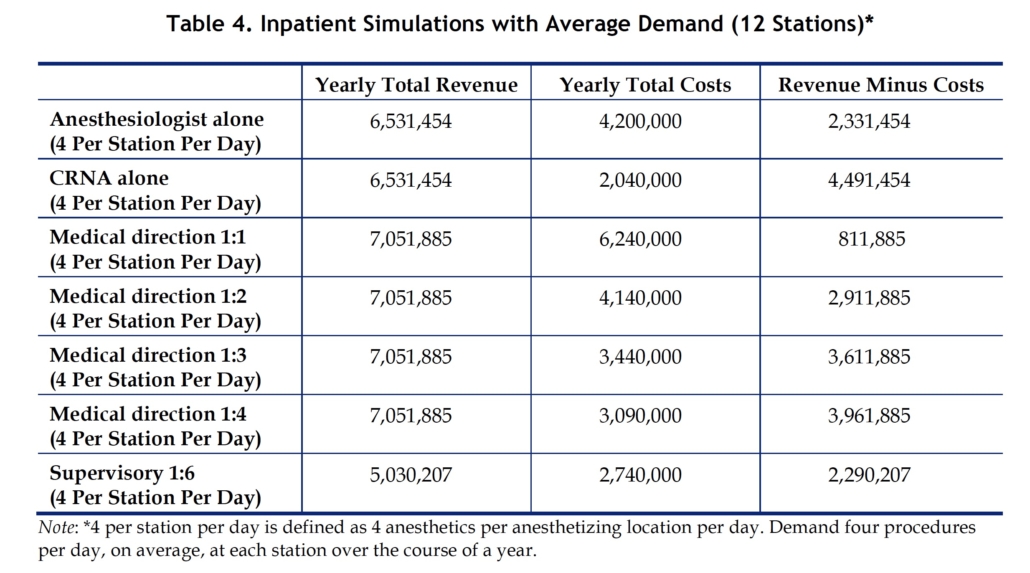
So, based on the chart above why wouldn't any CEO/CFO/CMO keep the physician Anesthesiologist in the loop? When I analyze the graph above I come away with a different conclusion: CRNA ONLY model isn't worth it for the savings. You don't get a "supervisor" or physician involvement in the care of surgical patients.
Based on the acuity of the cases the graph above actually validates the 1:4 model as very cost effective if you actually care about patient quality.
Can you explain why 1:6 generates less revenue?
Or why is 1:1 generates more revenues than MD alone?
Or also why the anesthesiologists costs 2million more per year compared to the CRNA?So, based on the chart above why wouldn't any CEO/CFO/CMO keep the physician Anesthesiologist in the loop? When I analyze the graph above I come away with a different conclusion: CRNA ONLY model isn't worth it for the savings. You don't get a "supervisor" or physician involvement in the care of surgical patients.
Based on the acuity of the cases the graph above actually validates the 1:4 model as very cost effective if you actually care about patient quality.
Or also why the anesthesiologists costs 2million more per year compared to the CRNA?
Right. So its a bullsh1t table that Blade posted.“Table from The Lewin Group, prepared for American Association of Nurse Anesthetists” - that tells you everything you need to know!
A LOT of assumptions are baked into this. 1:6 presumably billing less due to supervision modifier. Why the solo MD isn’t billing more is unclear. Why more is billed for supervision also isn’t clear. And I am puzzled at the idea that solo CRNAs are going to work for less than half the hourly rate of the MDs. So basically this is garbage propaganda.
Right. So its a bullsh1t table that Blade posted.
They're absolute experts at lying to anyone who will listen.The biggest con in the AANA’s playbook is that independent CRNAs are cheaper than physicians because of taking the average salaries of the two and comparing them. They know legislators have no idea how anesthesia billing works, and they’re fine with straight up lying to them.
That "table" is pure propaganda. I posted it because you all need to see what they present as fact. CRNA salaries are on the rise and the hourly rate is quickly approaching $140 per hour if not even higher. In addition, they expect a limited work week with set hours.They're absolute experts at lying to anyone who will listen.

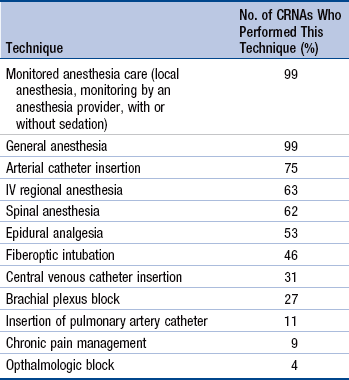
I'd be interested to see what percent of anesthesiologists are doing all those things. I know partners that can't do central lines. I've never met a crna that outright doesn't do spinals.
…I've never met a crna that outright doesn't do spinals.
I'd be interested to see what percent of anesthesiologists are doing all those things. I know partners that can't do central lines. I've never met a crna that outright doesn't do spinals.
@epidural man could you try and describe what specifically you think an anesthesiologist brings to the table maybe in using specific situations?
Not really.@epidural man could you try and describe what specifically you think an anesthesiologist brings to the table maybe in using specific situations?
@epidural man could you try and describe what specifically you think an anesthesiologist brings to the table maybe in using specific situations?
@epidural man could you try and describe what specifically you think an anesthesiologist brings to the table maybe in using specific situations?
I'd be interested to see what percent of anesthesiologists are doing all those things. I know partners that can't do central lines. I've never met a crna that outright doesn't do spinals.
Perhaps you should get out more.
Dear EpiduralNot really.
I think the market should decide though. That Wisconsin hospital needs to be open and honest about what they have done - and patients should make the decision.
When the housing market declined in 2008, the sellers agent colluded with the buyer and buyers agent agains the seller of the home prices. That means 3 against one seller in order for the transaction to proceed. The sellers agent has a financial incentive to depress the sale price in favor of the buyer in a difficult 2008 recession.
Since their commissions are a percentage of sale price, both sellers’ and buyers’ agents are generally incentivized to get the highest sales price. I supposed it’s possible that there can be collusion to get a lower sales price if it looks like the deal would otherwise fail.
The answer is actually our friends with a J.D. and father time. Once the bad outcomes happen, and they inevitably will in greater number when CRNAs are working on their own compared to anesthesiologists, it is the malpractice and sub-standard of care outcomes that will drive change. The CEO might think they are "saving" a small % of their budget by going with the cheaper (and inferior) option in straight CRNA care. In actuality, it only takes 1 successful lawsuit to undo multiple years of "savings." Yes that CEO/CFO/COO might not be there to take the brunt of it, but the med mal claims and thus insurance dues will go up for CRNA only care and eventually that will be the great mitigator.I have a question.
Are anesthesiologists better than CRNA's (as a group..obviously there are horrible anesthesiologists and great CRNA's)?
Because I believe - yes they bring something to the table that CRNA's can't bring. I could be wrong, but I believe it.
So IF that is the case - then when someone posts a news story that an entire hospital went 100% CRNA - instead of talking about what a travesty it is, and how we are screwed, or how we need to come up with another way to rape other human beings by scrapping tons of money of their hard labor (who will eventually turn around and do the same thing CRNA's do) -
instead of doing that - when we read of that hospital....the proper response is to laugh and laugh and say...."Ha. Good luck with that" and when that hospital comes back to an anesthesiologist....we have to band together...no matter how much they eventually offer...and say "F$%K YOU! Good luck."
But the way most of you talk is like you don't believe what I believe.