You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
3D hippocampal avoidance
Started by RickyScott

Nice
That's clever. I'd still try to get the IMRT plan going because you're going to spare a lot more than just hippocampus like this.
One other thought: that's a really low inferior border. How much parotid are you getting in there?
Also, if anyone from Evilcore is reading this thread DON'T GET ANY IDEAS!
One other thought: that's a really low inferior border. How much parotid are you getting in there?
Also, if anyone from Evilcore is reading this thread DON'T GET ANY IDEAS!
Advertisement - Members don't see this ad
That's also brain (non-hippocampal) sparing WBRT. Or very, very large partial brain RT. Seems reasonable for a fraction or two before you convert them to IMRT, though I suppose.
If someone is inpatient for brain mets (unless like a rare new diagnosis, but then the role of 'emergent' WBRT makes me concerned) I usually don't do HA-WBRT.
Curious as to the clinical scenario in this patient.
If someone is inpatient for brain mets (unless like a rare new diagnosis, but then the role of 'emergent' WBRT makes me concerned) I usually don't do HA-WBRT.
Curious as to the clinical scenario in this patient.
We can turn around an HA-WBRT plan in a few hours. I still do it as an inpatient. My dosimetrists and physicsts haven't killed me... Yet.
young pt w/ colon cancer, who wants aggressive care. Will have difficult time controlling gross disease.That's also brain (non-hippocampal) sparing WBRT. Or very, very large partial brain RT. Seems reasonable for a fraction or two before you convert them to IMRT, though I suppose.
If someone is inpatient for brain mets (unless like a rare new diagnosis, but then the role of 'emergent' WBRT makes me concerned) I usually don't do HA-WBRT.
Curious as to the clinical scenario in this patient.
We can turn around an HA-WBRT plan in a few hours. I still do it as an inpatient. My dosimetrists and physicsts haven't killed me... Yet.
If they haven't said it to your face, based on the interactions with my dosimetrists here and getting to hear the inside scoop on their issues with the attendings, I can all but guarantee they're talking smack behind your back.
Even for inpatients we usually give them 1-2 days for IMRT turn around. Maybe our dosimetrists are busier than yours?
young pt w/ colon cancer, who wants aggressive care. Will have difficult time controlling gross disease.
Looks like 7-8 brain mets? Assuming the giganto one (assuming it's all one lesion) in frontoparietal region is causing symptoms? Control rates for colon cancer with WBRT likely to be relatively poor IIRC the spectrum of radioresistance well - any consideration of surgery for symptom control then multi-lesion SRS?
do you have standard beam arrangement/optimizations?We can turn around an HA-WBRT plan in a few hours. I still do it as an inpatient. My dosimetrists and physicsts haven't killed me... Yet.
do you have standard beam arrangement/optimizations?
Two of our dosimetrists are very used to running these plans. The one who does it most often is doing 2 co-planar arcs and 2 90 degree couch kick arcs.
Advertisement - Members don't see this ad
I hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
OP could at least change the thread titleI hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes

I hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
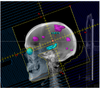
added an extra collimator sup and inf on hippocampus from picture and have mean dose of 5 Gy. Def blocking some brain, some of which is also not effectively treated with IMRT.I hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
Emergent inpatient IMRT is not cool. Signals disdain for billers and physicists also.
Sent from my iPhone using Tapatalk
?
I hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
but you can SRS that later if needed right ?
beautifulinpt ; had to start emergent whole brain xrt
even better: just put a margin around the lesions and come in with the SRS a few fractions later
provocative and true: a well-functioning dept should be able to go from sim to HA-WBRT getting tx on table in 3 hours or less, esp if one skips QA before the first fx.
My theory on this is charge the IMRT plan that day 1. No consult, no devices, nothing. Just the plan. JUST THE PLAN. (And skip QA, for the physicists.)Emergent inpatient IMRT is not cool. Signals disdain for billers and physicists also.
Sent from my iPhone using Tapatalk
Then bill whatever and however you want on day 2 and so on and so forth.
If people can live with that, if they can see that the beggars for clinical superiority can't be pecuniarily choosy and that's ok... then you're good.
But obviously, many are not good with that.
gangsta/inpt ; had to start emergent whole brain xrt
Yeah I know. I knew I had some issues, but I never knew just how bad a person I was until this thread
Can someone please explain to this hopeless academic why it's so horrible to deliver rapid IMRT?
I guess we can ignore for now that I generate new IMRT plans in 30 minutes every day on an MRI-linac.
Advertisement - Members don't see this ad
but you can SRS that later if needed right ?
Well sure but then why not just shift your MLCs to do something like below? You can SRS that later if needed, right? Excuse the poor block angles - paint doesn't let me rotate at anything other than 90 degree angles.
Similar to breast-sparing mastectomies, the closest analogy in radiation oncology - brain sparing whole brain.
If you're going to partial brain, then just do partial brain (which I wouldn't). Again, it's fine for a treatment or two until you transition to IMRT, but would not do a full 10 treatment course like OP did.
And this is STILL chopping down a tree to get 7 apples. Yet creating less entropy than the original fields 😉Well sure but then why not just shift your MLCs to do something like below? You can SRS that later if needed, right? Excuse the poor block angles - paint doesn't let me rotate at anything other than 90 degree angles.
Similar to breast-sparing mastectomies, the closest analogy in radiation oncology - brain sparing whole brain.
If you're going to partial brain, then just do partial brain (which I wouldn't). Again, it's fine for a treatment or two until you transition to IMRT, but would not do a full 10 treatment course like OP did.
View attachment 310479
beautiful
even better: just put a margin around the lesions and come in with the SRS a few fractions later.
Just did your lesion plus margin on a patient today due to mri delays! (although didn't include the edema 🙂 ).
Kobe looked at Jordan and said “You’re pretty good but here’s where I can do it better.”Just did your lesion plus margin on a patient today due to mri delays! (although didn't include the edema 🙂 ).
In the earlier days, I have done similar things when treating with WBRT but only as a boost. I prescribed 10 x 3 Gy to the whole brain and then boosted the cerebellum only with 3 x 3 Gy for instance in patients who came in with only cerebellar metastasis.
This all happened in the earlier days, when we would only SRS solitary lesions and a patient with 3-4 cerebellar metastasis meant automatically WBRT.
Actually this 3D-hippocampal sparing technique has been published before... The very first mention was in rats!

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
This all happened in the earlier days, when we would only SRS solitary lesions and a patient with 3-4 cerebellar metastasis meant automatically WBRT.
Actually this 3D-hippocampal sparing technique has been published before... The very first mention was in rats!
A precision 3D conformal treatment technique in rats: Application to whole-brain radiotherapy with hippocampal avoidance - PubMed
A novel approach for conformal microradiation therapy using 3D-printing technology was developed, implemented, and validated. A workflow was developed to generate accurate 3D-printed blocks from registered high-resolution rat MRI atlas structures. Although hippocampus was spared with this...
pubmed.ncbi.nlm.nih.gov
Kobe looked at Jordan and said “You’re pretty good but here’s where I can do it better.”
i know youve gone over it before, but what's your method again? thanks
Many times the patient with one brain met, or maybe two or two-plus etc, will have some sort of neuro compromise. And one will want to be getting the RT started right away, but WBRT is gauche, right? And "urgent," same-day SRS is kind of difficult. And there's some data that SRS upfront in neuro-compromised patients isn't the best. And maybe as Reaganite says you don't have an MRI yet...i know youve gone over it before, but what's your method again? thanks
So if you add all the aforementioned together, and keep in mind that WBRT+SRS patients had better long-term "brain control" on the whole, what seems reasonable is getting some partial brain to the lesion(s)+edema. If I treat the CT-edema areas the lesions are in there, and once I have an MRI and do SRS targeting my partial brain approach will have covered the targets. I almost always do 15 Gy/6 fx IMRT (to lesions+edema plus around 0.5cm PTV... again, the idea is cover to hedge and cover to be non-surprised once there's an MRI, and also to hark back to WBRT-ish volumes a little... call me sentimental). Some benefits of this are lesion shrinkage pre-SRS and oft times neuro sx decrease. Within a week after the 15 Gy is complete, come in with 18-24 Gy SRS single shot (depn on lesion size of course). Think of it as an updated, labor-efficient riff on WBRT+SRS (and it's ~0-5 Gy max to the hippocampus usually... and you don't even have to bother contouring it).
I actually fully agree with this.Well sure but then why not just shift your MLCs to do something like below? You can SRS that later if needed, right? Excuse the poor block angles - paint doesn't let me rotate at anything other than 90 degree angles.
Similar to breast-sparing mastectomies, the closest analogy in radiation oncology - brain sparing whole brain.
If you're going to partial brain, then just do partial brain (which I wouldn't). Again, it's fine for a treatment or two until you transition to IMRT, but would not do a full 10 treatment course like OP did.
View attachment 310479
Advertisement - Members don't see this ad