- Joined
- Jun 17, 2014
- Messages
- 63,099
- Reaction score
- 154,727
Me? I'm a little snarkier than usual, I suppose. Quarantine is getting to me a little. All in fun.I’ve followed blades posts for a long time on this site.
Are you doing ok man? This whole thing sounds like someone has logged in under your name and posting stuff. Just doesn’t seem like you.
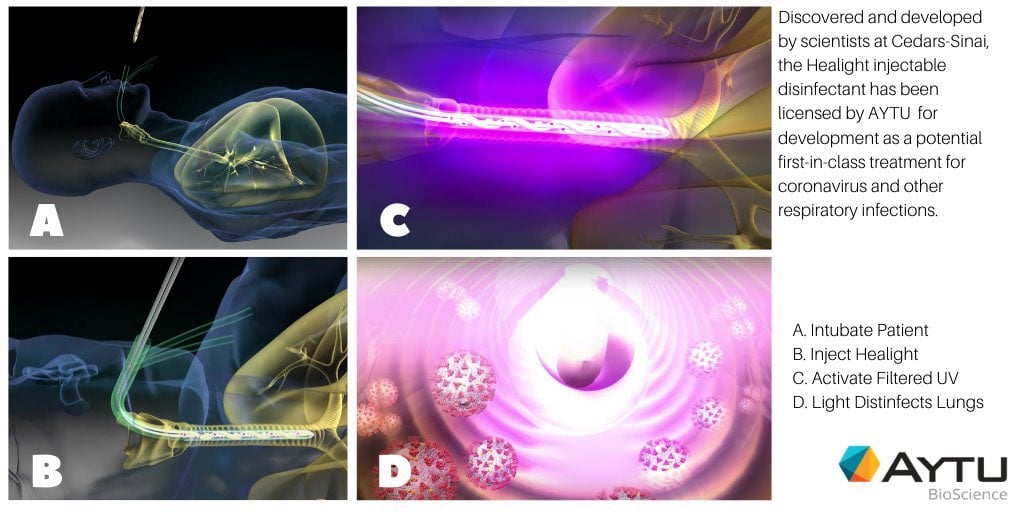
This is the most insane thing I’ve ever seen. Absolutely zero chance of this doing anythjng.Help!! Any ICU doctors using UV light with ETT? This company makes it, <link deleted by mod>
Does it work? Where can I buy? I think it looks interesting and helpful!
I went and looked at the paper, all bull****. Some stupid bioinformatics paper. Couldn’t follow half of the “conclusions” they were coming up with.There was a paper the Chinese put out. It’s in the CCM forum under “Are we treating ARDS” I believe. Interesting stuff.
Me? I'm a little snarkier than usual, I suppose. Quarantine is getting to me a little. All in fun.
This is the most insane thing I’ve ever seen. Absolutely zero chance of this doing anythjng.

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
Ok. Well, then that is your opinion. Don’t shoot the messenger. Just directing you in the proper direction.I went and looked at the paper, all bull****. Some stupid bioinformatics paper. Couldn’t follow half of the “conclusions” they were coming up with.
I stand by what I said, nobody has any idea about the pathophysiogy of hypoxia without poor lung compliance in these patients, except for the fact that nothing we’re doing is helping.
If I were any sort of outsider, medical or not, and I were reading this thread I’d think anesthesiologists were bat-**** crazy.
I’m concerned about @BLADEMDA. I was a little worried before the Dr. Oz post, now I flat out have concerns. Seriously dude, let us know you’re okay.
I'm missing the action!! I figure I would revisit my favorite old forums. I want to add my 2 cents so no flaming please :- Let me add a few things: No matter what you believe your government as a whole has let down the medical community. (Left and Right) The data/true numbers are hard to say. HOWEVER: the virus is highly virulent/contagious but NOT highly deadly. The worst places are obviously in big cities due to population density (gee wiz) Despite whatever you guys believe/feel all coronaviruses are seasonal. They are highest in winter/lowest in summer. There is a latitude effect just like flu etc. It will get better now in the Northern Hemisphere because we are moving towards summer and the UV index continues to increase. Trump is a clown but the weather/UV will now mild the storm. I suspect it will come back worse next time because it will be true winter (like when it started in China) vs our early outbreaks. Any vaccine created I suspect will not be great as all past data/attempts at making a vaccine (since SARS) have not been great. I practice anesthesia to pay my bills but I also practice other forms of medicine for health/longevity with a colleague. The medical paradigm in the U.S. IMHO is very flawed and all based on Pharmaceuticals. You have to do your own homework when it comes to treatment/studies etc... The CDC/FDA is a prime example during this pandemic. I do believe that the antimalarials and azithromycin have some positive effect WHEN and ONLY when given early in course. Do you guys know howthe virus works? The virus attacks hemoglobin (beta chain) which kicks out the heme in the red blood cells. What happens....? 02 is unable to be delivered to the mitochondria. Hmmm why is that important? Well heme synthesis first begins in the.... Mitochondria. So without getting fancy the virus knocks off the heme which decreases the rbc's ability to carry 02. Why do antimalarials work? Because covid-19 like malaria inactivates the rbcs to carry 02 to mitochondria. The blood phenotype of a Covid-19 pt somewhat resembles that of a pt infected with Malaria. Antimalarials are beneficial if given at the RIGHT time aka early. When a patient is shot up in the ICU it is to late.The time would be as patient develops symptoms but before they have respiratory failure/compromise. I'm sure you guys have read/heard about the ACE2 component of the virus right? Well chewing nicotine gum (obviously don't smoke) will decrease the expression of the ACE2 receptor component of the virus attaching/entering cell mechanism. This is a helpful treatment AGAIN early on. Not when you can are barely breathing/in the hospital. You won't hear this from the media or Faucci/Berk etc.... What about the MARIK protocol?... That is high dose iv vit c with iv thiamine +/- steroids in ICU/sepsis patients. That would be helpful too but only some big academic places are doing it... Why? IV VIt C is not very profitable for big Pharma. I'm sure you guys know the antimalarials are quite cheap/old....... not as profitable either :0 You bring up the thrombosis issue which again is not about age it's actually very simple. When heme proteins liberate iron it leads to....CLOTTING (now magnify this on the scale that it is in happening in a hospitalized covid patient) The body is releasing massive iron/Ferritin because of the continued destruction of the HGB/rbc's. You will see every hospitalized covid-19 patient with high LDH/Ferritin levels. Social distancing is one thing, but to tell people not to go outside where you can help your body generate immunity is quite silly. The virus spreads very easily indoors but outdoors in natural light lessons the effect. Generating Vitamin D via the sun will do that....Lastly whether you believe it or not this virus would have ran it course based on timing/seasonality. Here are a few links since everybody needs "evidence".

Predicted Inactivation of Viruses of Relevance to Biodefense by Solar Radiation
UV radiation from the sun is the primary germicide in the environment. The goal of this study was to estimate inactivation of viruses by solar exposure. We reviewed published reports on 254-nm UV inactivation and tabulated the sensitivities of a wide ...www.ncbi.nlm.nih.gov
Inactivation of the coronavirus that induces severe acute respiratory syndrome, SARS-CoV - PubMed
Severe acute respiratory syndrome (SARS) is a life-threatening disease caused by a novel coronavirus termed SARS-CoV. Due to the severity of this disease, the World Health Organization (WHO) recommends that manipulation of active viral cultures of SARS-CoV be performed in containment...Effect of ultraviolet germicidal irradiation on viral aerosols - PubMed
Ultraviolet (UV) germicidal air disinfection is an engineering method used to control the airborne transmission of pathogenic microorganisms in high-risk settings. Despite the recent emergence of respiratory viral pathogens such as SARS and avian influenza viruses, UV disinfection of pathogenic...
Indoor transmission of SARS-CoV-2
Background By early April 2020, the COVID-19 pandemic had infected nearly one million people and had spread to nearly all countries worldwide. It is essential to understand where and how SARS-CoV-2 is transmitted. Methods Case reports were extracted from the local Municipal Health Commissions...www.medrxiv.org
Please don’t tell me you actually eat at Taco Bell.1. Vit D- that means 2 glasses of milk per day to me
2. Vit C- that means a glass of orange juice or a multivitamin to me
3. High dose H2 blockers IV- that means a pepcid tablet twice per day especially after taco bell or pizza
4. Nicotine Patches- I'll pass as I don't smoke
5. UV light- that means exercise outside in the sunlight if possible without a mask
That's as far as I would take any of the junk science surrounding Covid 19. I am awaiting the trial data on HCQ for mild/moderate disease.
I also fully expect Remdesivir to show efficacy if used early in the infectious process.
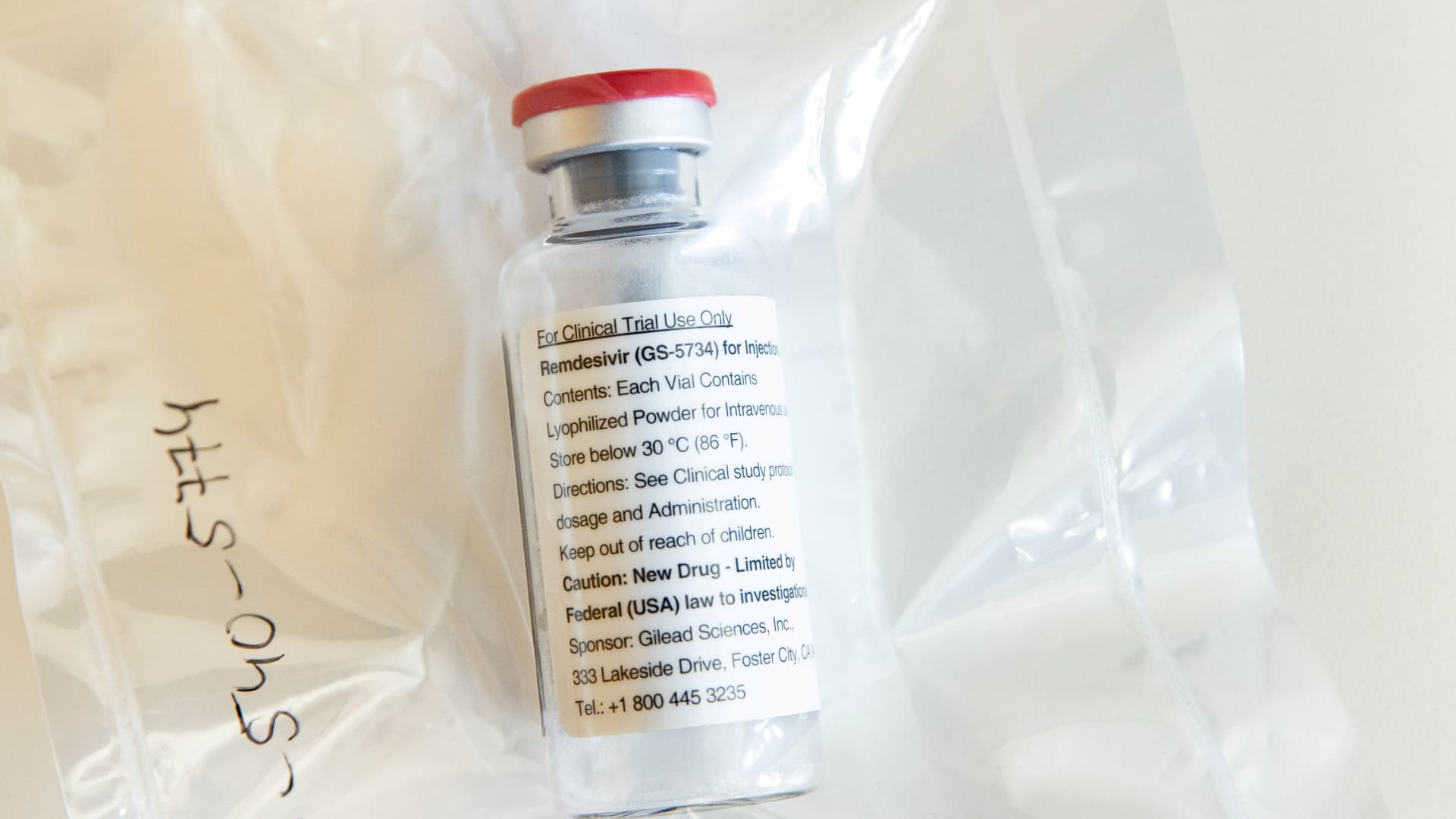
Gilead says early results of coronavirus drug trial show improvement with shorter remdesivir treatment
Gilead Sciences said preliminary results of a coronavirus drug trial showed at least 50% of patients treated with a five-day dosage of remdesivir improved.www.cnbc.com
1. Vit D- that means 2 glasses of milk per day to me
2. Vit C- that means a glass of orange juice or a multivitamin to me
3. High dose H2 blockers IV- that means a pepcid tablet twice per day especially after taco bell or pizza
4. Nicotine Patches- I'll pass as I don't smoke
5. UV light- that means exercise outside in the sunlight if possible without a mask
That's as far as I would take any of the junk science surrounding Covid 19. I am awaiting the trial data on HCQ for mild/moderate disease.
I also fully expect Remdesivir to show efficacy if used early in the infectious process.
Gilead says early results of coronavirus drug trial show improvement with shorter remdesivir treatment
Gilead Sciences said preliminary results of a coronavirus drug trial showed at least 50% of patients treated with a five-day dosage of remdesivir improved.
This is the most insane thing I’ve ever seen. Absolutely zero chance of this doing anythjng.
You sounded good, and I mean normal level @BLADEMDA good, and then you linked a CNBC article with a Gilead stock photo and an article telling us Gilead thinks their drug is pretty sweet. Thanks dude. We are fuggin' scientists. Can't we at least pretend to act like it?
And yeah, at least go to Chipotle.

I think it's insane to eat mould to kill bacteria inside body. Oh wait, what's this?? Penicillium - Wikipedia
Looks like censorship of medicine research!! https://www.wsj.com/articles/an-experimental-ultraviolet-light-treatment-for-covid-19-takes-political-heat-11588005938

I believe plasmapheresis has been working....... Covid does resemble high altitude sickness... Absolutely ! French are doing the trial now with the nicotine :0 You don't have to agree with anything I am saying. In fact I want you to research for yourself. I am just giving you some perspective and information that seems to support certain things. Everyone needs to do homework :0 You cannot deny the latitude/Vit D effect. As you probably guesses I suppot the natural way. Taking a pill or supplement is not the same as doing it the real way. All flus/coronavirsuses are seasonal and seem to go down in the summer.....Light and the biophysics of it are quite complicated. I'm not sure about that device, but old school UV blood irradiation would def work since you can't put the patients outside :0 Blade you are in the south. Just get your butt outside i'm sure you don't live in a little shack :0
The Nobel Prize in Physiology or Medicine 1903
What do you think now with the NIH randomized control trial showing efficacy?You keep bringing up their "preliminary" studies as if they're impressive or something. It's a garbage study, that's why it's getting trashed. Not only is there no control group, but the patients in the study are not patients who would be statistically expected to die anyways. Based on the stat article, look at how they define the "severe" patients they are studying: "severe" excludes "patients w multi-organ failure, abnormal liver tests, moderate kidney disease, needing mechanical ventilation at time of first evaluation, needing mech ventilation for 5+ days." The patients they are studying are basically patients who have fevers lol. These are not sick patients. And since this isn't data from a controlled trial, there is literally 0 information you can gain from it about the drug's efficacy. A drug that is highly effective does not need a large sample size. Bigger randomized sample sizes are needed when you want to validate small differences. Another thing not mentioned is how they changed several endpoint goals in the middle of the study. This, like raising the sample size, is a move to compensate for low power. It's pretty obvious what they're doing. I'm not saying this drug can't work. You just won't be able to tell from this study.
Also, just from a logical standpoint, do ppl realize this drug was originally created specifically for a different virus, and it failed? Ppl are hoping this will be a miracle drug for a virus which literally did not exist when it was designed. Think about the odds of that happening. Has there ever even been a drug which has successfully been repurposed for a virus? I can't think of one.

I'm blown away. Amazing data. The efficacy is so good, it's mind boggling. We found the miracle drug we have all been waiting for. It's time to re-open everything, everywhere. Dust off your bball shoes, Kevin Durant. It's time to hoop.What do you think now with the NIH randomized control trial showing efficacy?

NIH Clinical Trial Shows Remdesivir Accelerates Recovery from Advanced COVID-19
Hospitalized patients with advanced COVID-19 and lung involvement who received remdesivir recovered faster than similar patients who received placebo, according to a preliminary data analysis from a randomized, controlled trial involving 1063 patients, which began on February 21.www.niaid.nih.gov
If UV has any effect, it’s minimizing the virus’ viability duration on surfaces and in the air. Once infected, UV ain’t gonna do s**t.

 tringali-health.com
tringali-health.com
In seriousness, it looks like there may be some efficacy but it's not potent and nothing even close to what they first leaked. Recovery time lowered from 15 to 11 days. No statistically significant effect on mortality. A small step is a start tho. A viral disease like covid has never been successfully eradicated with a drug playing a big role. Given the fact that they excluded so many ppl in the trial and patients who died, the real world effect will likely be very small. They didn't even look at mortality as a primary outcome bc they changed the primary outcome to time to recovery once they saw that this drug wasn't a game changer.What do you think now with the NIH randomized control trial showing efficacy?
NIH Clinical Trial Shows Remdesivir Accelerates Recovery from Advanced COVID-19
Hospitalized patients with advanced COVID-19 and lung involvement who received remdesivir recovered faster than similar patients who received placebo, according to a preliminary data analysis from a randomized, controlled trial involving 1063 patients, which began on February 21.





The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro
Although several clinical trials are now underway to test possible therapies, the worldwide response to the COVID-19 outbreak has been largely limited…www.sciencedirect.com
ivermectin a possibility
PulmCrit- First placebo-controlled RCT on remdesivir for COVID-19
Remdesivir is being promoted as an anti-viral agent for the treatment of COVID-19. The first randomized, blinded, placebo-controlled trial ofemcrit.org
- Wang et al. is the first placebo-controlled, double-blinded, multi-center RCT of remdesivir. The study was stopped early due to poor recruitment after including 237 patients, but otherwise appears well designed.
- Remdesivir had no effect on any clinical or biological endpoint (including viral load).
- Lack of an observable effect could theoretically relate to delayed administration of remdesivir or underpowering of the study. However, this is a thoroughly neutral study that shouldn’t be mischaracterized as showing promise.
- Further RCTs will clarify what role remdesivir has in COVID-19, if any. This study suggests that remdesivir probably doesn’t confer major clinical benefits.
So, just to keep track of things. The following are what has been suggested (all the way up to PUSA in an extremely dangerous manner) as treatment/prevention. So far absolutely none of the following have good evidence for treatment or prevention of COVID19:
azithromycin, HCQ, plaquenil, remdesivir, famotidine, ranitidine, tocilizumab, ivermectin, vitamin C, vitamin D, UV light therapy, iron chelation, blood letting, any other manner of vitamin/OTC/mineral therapies that have been promoted as preventative.
What has worked? Conservative critical care medicine (limit IVF, oxygenate, ventilate, let the patient declare themself). ARDSnet protocols.
Anything else?
Where do ACEIs/ARBs fit in your list? I realize that if they worked, that should've already been seen given their widespread use. But the infection surrounding the ACE2 and another clinical paper (retrospective so still has biases. RCTs needed) showing their value got me thinking.
Where do ACEIs/ARBs fit in your list? I realize that if they worked, that should've already been seen given their widespread use. But the infection surrounding the ACE2 and another clinical paper (retrospective so still has biases. RCTs needed) showing their value got me thinking.
When this started we thought they may be harmful/a risk factor for severe disease.
Even if we didn't have any studies available, I would think we would know by now if there was a game-changing kind of therapy out there, simply bc of the fact that our wave lagged behind countries like China and Italy. For example, they've been using remdesivir for months. It was actually part of the ICU protocol in Italy since February. From their experience, they're saying that it seems to help some patients but have no effect in others. They've already told us they're not seeing significant benefit. If something stood out as very effective, they would have made it known.So, just to keep track of things. The following are what has been suggested (all the way up to PUSA in an extremely dangerous manner) as treatment/prevention. So far absolutely none of the following have good evidence for treatment or prevention of COVID19:
azithromycin, HCQ, plaquenil, remdesivir, famotidine, ranitidine, tocilizumab, ivermectin, vitamin C, vitamin D, UV light therapy, iron chelation, blood letting, any other manner of vitamin/OTC/mineral therapies that have been promoted as preventative.
What has worked? Conservative critical care medicine (limit IVF, oxygenate, ventilate, let the patient declare themself). ARDSnet protocols.
Anything else?
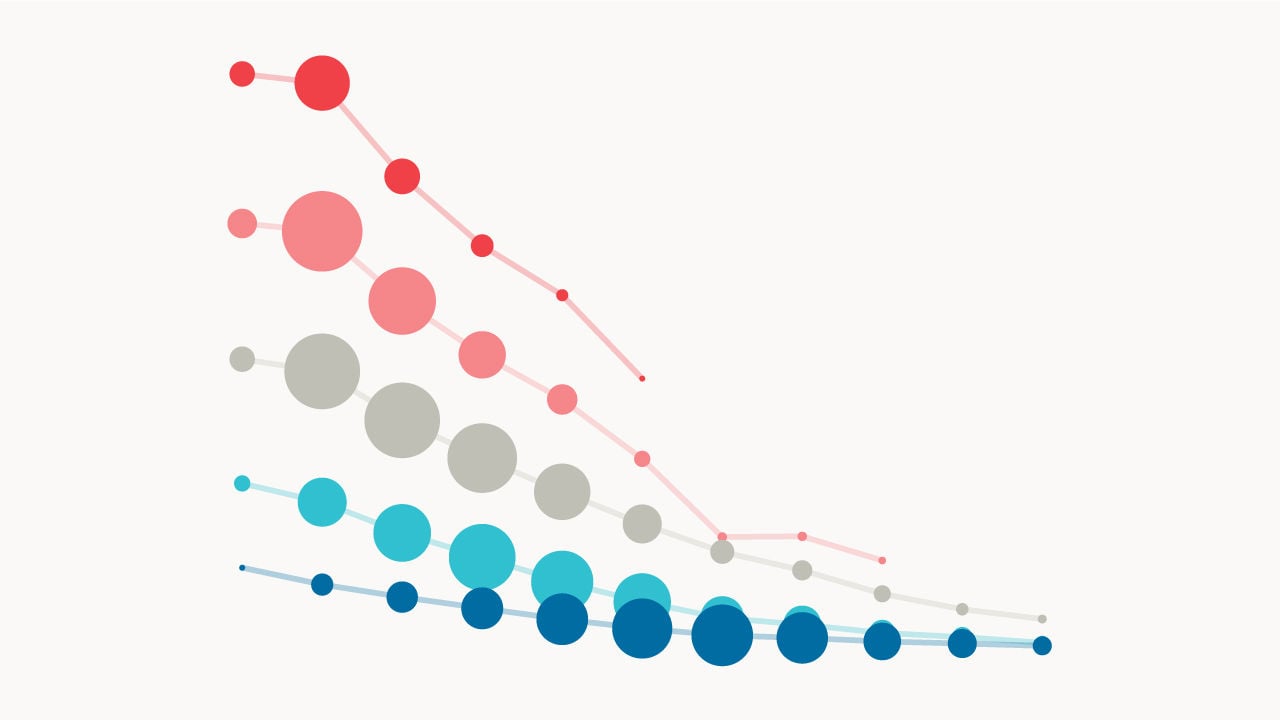
Average number of years lost per each covid death: 10-11 years
Per this study, "people killed by Covid had only slightly higher rates of underlying illness than everyone else their age."
View attachment 304747Would most covid-19 victims have died soon, without the virus?
A new study suggests notwww.economist.com

Remdesivir is fundamentally targeting viral replication machinery. Nothing else. It should in theory wipe out the virus but not change the damage done and that continues.
where is the viral load data from these studies. That’s what ultimately matters to judge Remdesivir effectiveness, not
Mortality.
You could kill off the virus and the
Millions of dead virus junk floating around is still stimulating a massive inflammatory and coagulation response probably For weeks..which is not going to stop mortality. The studies combining Remdesivir with potent anti inflammatory/anticoagulant will probably be the holy grail in terms of moving the needle with mortality.
I’ve seen this heme stuff floating around for some time, now. For what it’s worth from the biochem/cell bio perspective, the chloroquines appear to prevent fusion of the endosome with the lysosome, inhibiting entrance of the virus into the cell via the endocytotic pathway. Viral particles are visualized in large quantities in relatively massive endosomes, few particles are present in lysosomes, and few are present in the cytoplasm in in vitro studies of type II alveolar cells bathed in a medium with virus and either chloroquine or hydroxychloroquine. Chloriquine seems to be the more effective of the two. The virus can still enter via a nonendocytotic pathway. The conclusions regarding the mechanism of chloroquine with regard to Covid has little to do with its effect on RBCs, from what I remember. Though the authors admitted a poor understanding of whatever was happening. I don’t have the citation handy.Is the heme hypothesis is from a chemistry journal op ed or something that concludes “This paper is only for academic discussion, the correctness of the theory needs to be confirmed?” It says it’s “possible” viral proteins could “coordinate” an attack on porphyrins based on computer modeling ....
Also why wouldn’t we just do an exchange transfusion if this was “how the virus works.”
I definitely think we should put all ICU patients on >4 grams of vit C, enough vitamin D to cause obstructive uropathy, high dose nicotine patches on all 4 extremities to really ramp up their metabolic rate, expose their bare skin to high intensity UV light and Mojave like temperatures (even if already febrile). I’ve educated myself a lot on this as a side hobby and have it figured out.
While we are at it COVID also shares many symptoms with high altitude sickness (headache, shortness of breath, etc) may as well start them all on Diamox too. Seems to make sense.
From wiki: In modern usage, sophism, sophist and sophistry are used disparagingly. A sophism is a fallacious argument, especially one used deliberately to deceive. A sophist is a person who reasons with clever but fallacious and deceptive arguments.
We often let our imperfect reasoning deceive us before we know the true facts. What ever happened to evidence-based medicine and why are we replacing it with physician feeling or opinion? Or even worse, political opinion?
There is no holy grail. The Remdesivir RCT from China had lots of patients getting steroids.The studies combining Remdesivir with potent anti inflammatory/anticoagulant will probably be the holy grail in terms of moving the needle with mortality.
There is no holy grail.