Light at end of tunnel
Dangerous to be right when government is wrong
Removed
Lifetime Donor
5+ Year Member
- Joined
- Nov 16, 2016
- Messages
- 985
- Reaction score
- 984
This is not going to end well...

I am waiting for another thread titled: 'Do physical therapists respect MDs?'
What is the purpose of this thread?
Wow, where do I begin?!
1. You make it sound like NSGY consulting you should validate all of your inflated notions. Of course they are going to ask you how the pt is doing! It's your job to work with the pt on PT!!!! They are busy, oh you know, doing brain and spine surgery all day, so it's kind of understandable that they'll delegate physical therapy to the physical therapists and then ask how the pt is doing. You have no point at all by saying "neurosurgery LITERALLY consulted us today".
2. Bruh what? You're just trolling. You think that you guys have more in-depth general A&P "simply due to the fact" that we spend an extra 12 minutes reviewing depolarization before spending the rest of the semester learning anatomy? Are you kidding me? A&P at my school went more in depth than it did for our PT students. Our A&P exam also had nothing to do with muscle physiology or neuroscience - we had a separate class for that. Not to even mention that half of the people already took A&P in undergrad, and that muscle physiology is a required component for most gen bio classes and the MCAT. We dissected our cadavers from head to toe while our PT counterparts only did MSK. Who knows more anatomy?
3. You think EM docs use scribes to do medical work? Lol wut. Are you also comparing ED scribes to how other specialists use NP's and PAs? Go learn what an ER scribe does.
Didn't they superficially change your degree title from "Master of Physical Therapy" to "Doctor of Physical Therapy" to help your egos and your insomnia? Why are you calling MD's ' "doctors" '. I see the word "doctor" is still a trigger point for you. Your PT experience would make for a great personal statement story for your medical school application. You should consider going to doctor school!
Our school does the same thing with the dental students instead of PT like in your case. Despite being exposed to 80% of the material we are exposed to, their passing requirements are much lower and their questions on exams are much easier. They know they are not expected to absorb and learn a huge chunk of the material we are responsible for and that is reflected in their attitude and knowledge. I don't blame them for not wanting to memorize mechanisms for inborn errors of metabolism.
1. Yep, clearly our focus is purely on doing a quick procedure, keeping the patient alive, and that's it. No chronic treatment. We don't focus on that boring ****. We only do the sexy emergency procedures and let suckers like you do the "real" medicine. Like you said, its only your job to have emphasis on the healing processes. /s
2. DOs also make a minimum 2.5x the income than you do.
3. This is funny, I have to re-quote it here. "pain from nociception stimulation from the immune system". Who talks like that?! You are trying to hard. Stop trying to use redundant words, it exposes your ignorance. I'll be sure to remind my mechanic that 'my car goes forward due to the chemical reaction creating internal combustion inside the cylinders of my engine'.
4. Are you arguing that you guys know the pathophys concerning tropinin, hgb, hct, etc more than even a second year med student?!?!?! All because you have to have physical contact with the patient?!?! I have to smoke whatever you are smoking. My grandmother had a lot of physical contact with me as a kid while I was sick, I guess she was also required to know a ton about troponin levels. Ridiculous statements deserve ridiculous comebacks.
1. No you don't. You think you know what they really do, but reading wikipedia doesn't really make all the connections in your brain that you think you have. That is exactly why you can't legally inject it.
2. I can see why you are so self-conscious about defending your field now. With friends in MD, DO, DDS, PharmD... I'd also feel compelled to remind everyone that there is a "D" in DPT.
3. This is the only sentence that comes across as you being a genuinely decent guy. I realize my post is also harsh (this thread is inflammatory), so I can understand how in real life people may be different than how they come off on the internet. I wish there was more interaction between professional school students so that people wouldn't keep their misconceptions bottled up, but instead would have a lively discussion over dinner.
Old but confused. Why do pre health students comment on practices they are clueless about? We literally had NSG consulting us today on how a postop patient was doing in our session....
Let's clarify what @AlteredScale meant about with the admonishment to be respectful. This is not it.I'm not prehealth. And what we forget about is you, not the patient. The point is that no one but you cares about your inferiority complex and the chip on your shoulder
I understand.@Winged Scapula Im keeping this post objective and professional and just responding to points. Sorry for the inflammatory posts in this thread.
Have a nice rest of the weekend.
Hey guys! I'm obviously going into physical therapy as you can tell by my name. I just wanted to start of by saying I have great respect for physicians and I respect the amount of knowledge you have. I was wondering why a lot of physicians don't respect physical therapists. I know many do, but from what I have heard from many pts is that physicians aren't aware of the amount of schooling we go through now and the amount of knowledge we have in the rehabilitation setting. So I just wanted to ask the physicians who don't respect physical therapists a lot is why don't you? Thanks! P.S. I'm not trying to start a turf war or anything and I'm not trying to say pts are smarter than MDs!
Yikes..kinda proving his point here..there are instances where a physician may suggest a less than optimal PAM. For the patient's sake and for OUR code of ethics (yes they also include beneficence and non-maleficence) a PT or OT should communicate with the physician about this. It's not about control or power, MD's are scientists and have superior knowledge diagnostically no doubt- treatment wise outside of medical intervention- PT's, OT's, and SLP's have a wealth of knowledge that can facilitate a patient's best outcome.yeah, the physician knows more and is primary medical authority for that patient. On another front, they are also your customer as they control the referrals....it's best to keep the customers happy and stop assuming that it's disrespectful to disagree with you
Just a few thoughts:
1) PT/OT play rather different roles inpatient vs outpatient. One ends up being all about dispo and getting the right placement; the other about actually completing a course of therapy with specific goals in mind. Obviously the physician interaction with them will vary significantly between these arenas.
2) PT, OT, speech, etc, can be "black boxes" for many - things that get ordered but we have no idea what really happens. Definitely worth spending a couple hours with each of these as a student just to have a sense of what they do with a patient. It can be very helpful when you get recs back for a pt that don't make sense.
3) This is purely anecdotal, but at both my medical school and my current institution, all of the PTs and OTs were very young - as in the overwhelming majority were <30. I don't know whether this represents a lot of turnover in the field or simply a recent expansion of the field, but perhaps some ageism is at play too. I can imagine I would weigh the opinion of a 50 year old PT with decades of experience differently than I would that of a 24 year old.
") ......
......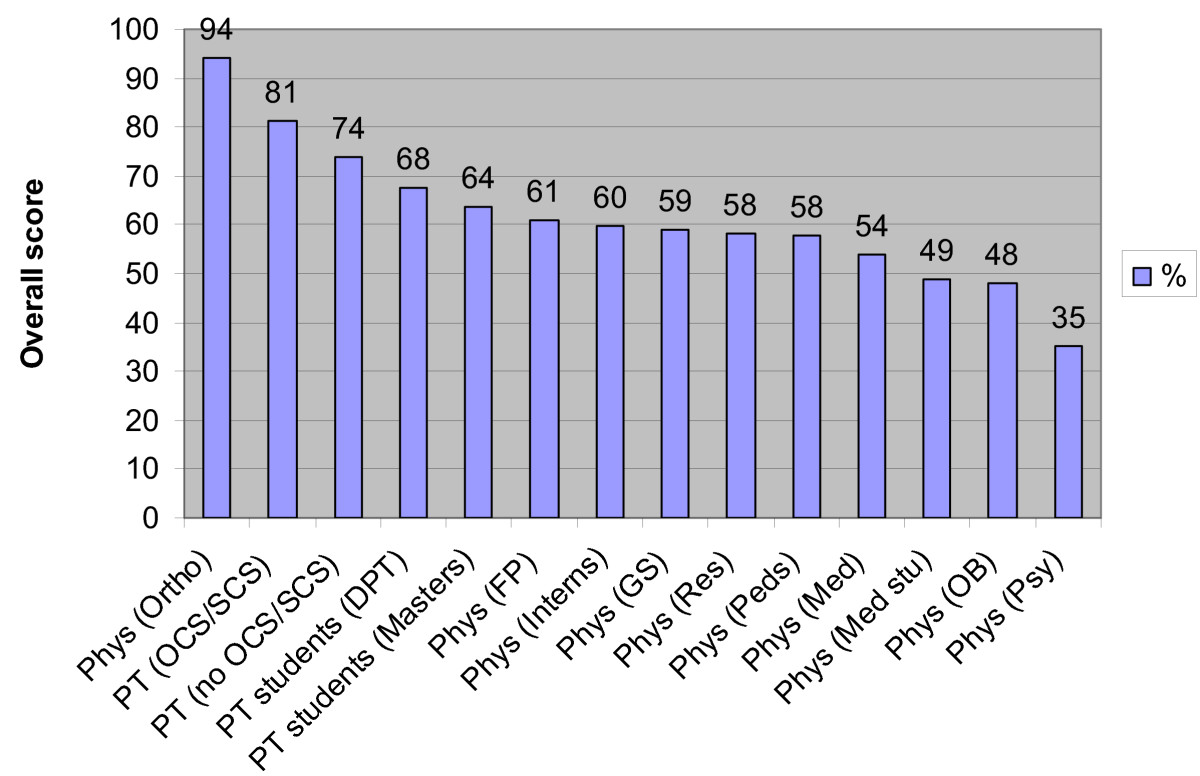
^I might be blind but you list other for radiology, anes etc, but i dont see Other on the chart..
I figure those 2 fields + EM should score pretty high since they deal with a ton of musculoskeletal stuff
I mean i treat most ppl with respect. It's another field and a very important part of teh treatment team.. we need a LOT more PTs. Most of them are pretty pleasant ppl and easy to work with. Out of all the co workers in the hospital, the only ones ive had issues with in the past were surgeons and nurses
.... I completely agree that I would hope radiology has greater education in this area as they deal with a ton of musculoskeletal issues.... The quote you are looking at is I believe from the "Figure 1." part that I included which I actually copied and pasted from the article which I linked to, mainly to give people a general description of the figure I included below that statement. While, like I said above, I 100% agree those in radiology should have a wide variety of Musculoskeletal knowledge and be very well versed in the anatomy/physiology, this article was mainly looking at not only the NUTS AND BOLTS of musculoskeletal anatomy/physiology but moreso, how to treat and manage musculoskeletal conditions which is where I believe PTs and those doctors in the orthopedic field are most well versed. Just like any specialized profession, I am simply trying to advocate that PTs now have to get their doctorate and although they didn't go to medical school, they are highly trained in areas that others may not. Just as I would hope that a general practitioner or orthopedist would refer out when a patient came to them with a new pregnancy/pregnancy concerns (i.e. refer to an OBGYN)..... I would hope that someone would refer to a PT, orthopedist &/or neurologist etc. for a Neuro-musculo-skeletal condition. Just because someone went to medical school does not automatically make them a "jack of all trades"... All professions and specialties have their limits and should know when to refer out....if not, then personally, I don't believe they are doing their job and are not putting their patients' issues/values first.
I'm saying I looked into both quite extensively....and yeah, the doc knows more
How does osteopathic manipulation compare in terms of scope of knowledge to what the majority of PT referrals cover? I guess, in other words, would training in OMM suffice for most basic PT referrals?
No--PT's will do some manipulation, but they're doing far more than just that. OMM can be very beneficial for patients, but it's typically not going to help alone with the long-term biomechanical changes needed to help with back pain, shoulder pain, or with helping regain function after a stroke.
None of the PTs I work with at our VA or academic center do just modalities (manipulation, ultrasound, dry needling, etc.). In private practice they do modalities more often, as you can bill for it and it keeps the patient coming back as they're typically things that will make you feel better temporarily. So then the group makes more money.
Appropriately trained PTs use modalities to better allow the patient to participate in the exercise program. If your shoulder hurts too much to work on scapular stabilization or RTC strengthening, then a PT might try heat/dry needling/US so that you can get a little more pain-free ROM to allow you do do those exercises.
The same goes for us--if I see a patient in clinic and RTC dysfunction/RTC impingement, then I may do a steroid injection. Sometimes that alone fixes the problem because the patient will use the shoulder more, but often they need at least a short burst of PT and a good home exercise program to correct the biomechanical deficits that lead to the problem in the first place. The injection helps them work with PT, but the PT is what will provide them with the long-term relief.
As a physiatrist, if PT's disappeared, it'd be as bad as if an oncologist lost all access to radiation/chemotherapy. OK, well, our patients wouldn't die, but my point is it's a mainstay of PM&R treatments.
(Lets not forget OT and SLP, though for outpatient MSK issues most of our referrals are to PT)
No, it’s really not. My girlfriend is going to PT school and I study with her daily. It’s not the same. I understand this is your wife and you’re naturally biased, but what you’re saying is simply not true.My wife is a PT and from I've seen of their curriculum, it is comparable in difficulty, even though admittedly different in scope. But, for instance, my med school has a good majority of neuro taught by two DPTs, and the slides we got were the same as the PT program's neuro class.
Do optometrist really make as much as MDs? I did not know that. I’ve made a huge mistake.What is up with this thread?
Who gives a crap about any of this? The issue isn't whether MDs "respect" you. It's whether your PATIENTS respect you. What does "respect" even mean in this context?
I am an optometrist and that makes me one of those "not a real doctor" doctors. My standard response to this issue, which actually hasn't even come up in years has always been that when people ask or accuse me of not being a real doctor, I say "You're right. I'm a doctor like Julius Irving is a doctor but I get paid like a real doctor so I'm totally cool with it."
Here's what I've learned after 17 years in this business:
Some MDs will respect you because you take good care of their patients, you communicate well with them and you are easy to deal with.
Some MDs will NEVER respect you no matter how many people you make an obscure diagnosis on, how many people's problems you solve, how well you communicate or really what you do and there ain't a damn thing you can do about it so you just move on with your life.
I have a good network of local ophthalmologists, neurologists, GPs, rheumatologists, allergists and other people that I work with and I just deal with them. The maniacs and the bad mouthers, I don't deal with. It's that easy.
Honestly.....this is such a NON-issue. At least for me it is.
You're nothing more than a glorified yoga instructor. This is based on first hand experience from PT treatment.
It's not true that some of the curriculum I've seen with my own eyes is literally the exact same? Lol.No, it’s really not. My girlfriend is going to PT school and I study with her daily. It’s not the same. I understand this is your wife and you’re naturally biased, but what you’re saying is simply not true.
It's almost as if your girlfriend, you, his wife, and he all go to different schools and so comparisons between 2 different pairs of them might differ!No, it’s really not. My girlfriend is going to PT school and I study with her daily. It’s not the same. I understand this is your wife and you’re naturally biased, but what you’re saying is simply not true.


We are a loving family here...Man, I should wonder over to the MD forums more often... Mods on this side of the fence allow for much more heated/inflammatory threads!
I think I'll stay in the pre-MD forums until MS1 though
Now, back to lurking...
Lol then hopefully I get to join soon!We are a loving family here...
Do optometrist really make as much as MDs? I did not know that. I’ve made a huge mistake.


