SLUsagar said:
unlike yourself senor ANDY, i truly am a proud ******...
what's the Dx on your pics???
I feel like a ****** today. Missed a focus of obvious LSIL when I previewed one of my slides last night.
You cought the LSIL on the other slide but you missed this???.
Quite embarrassing. I am a ******. And I'm damn frickin' proud of it! Dehhhh.
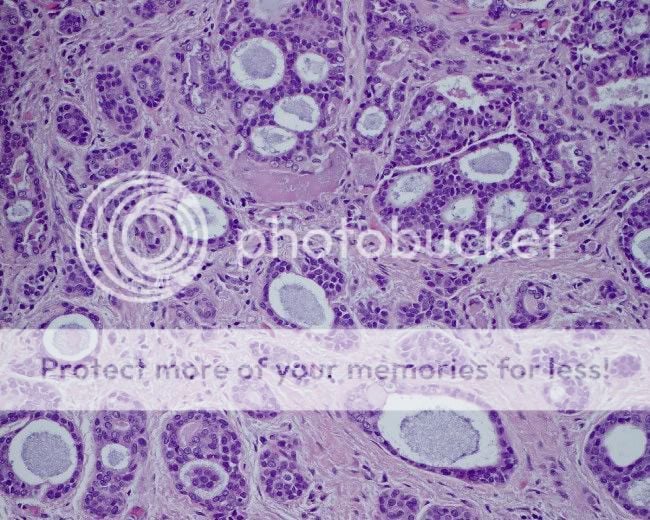
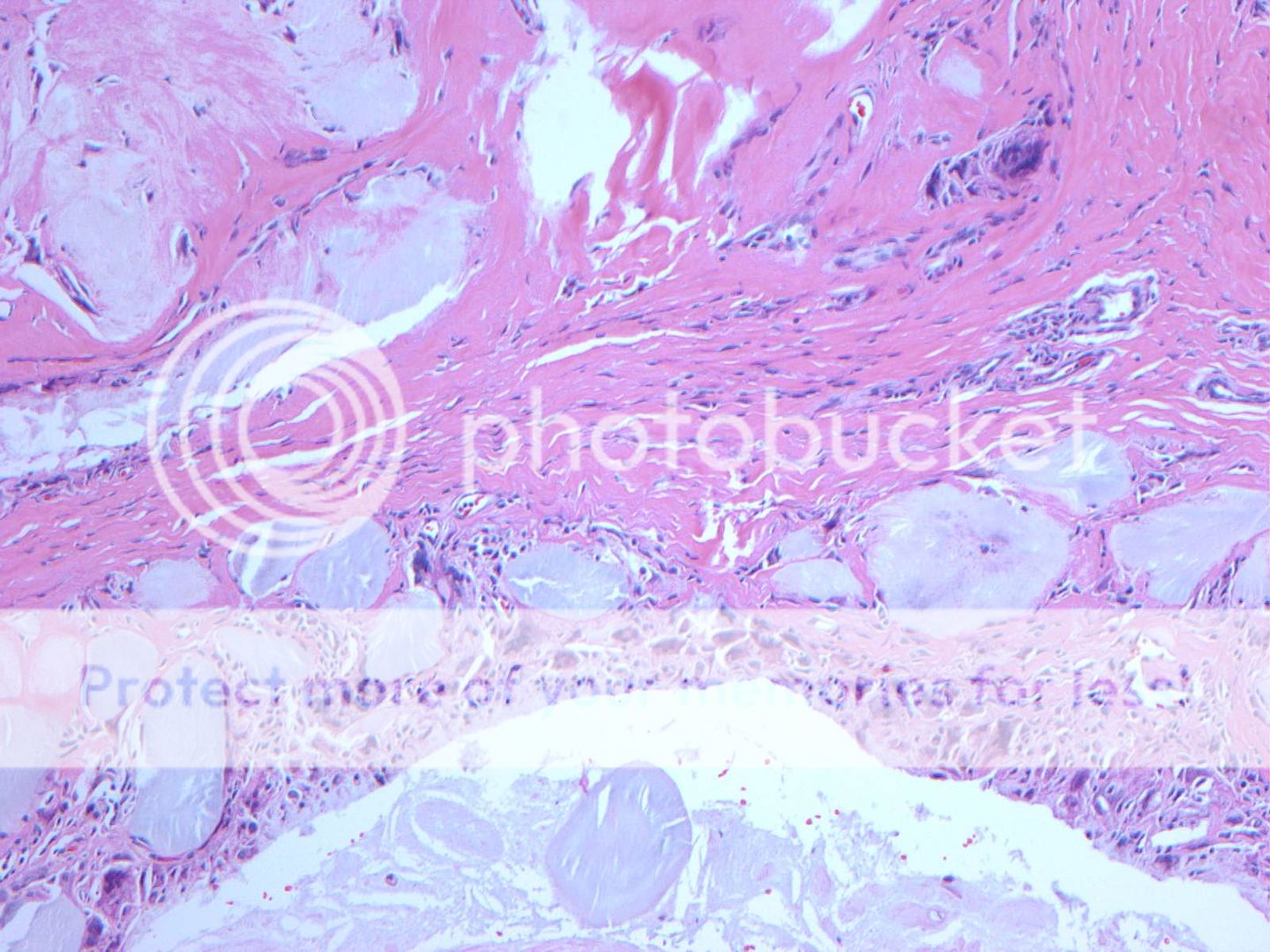
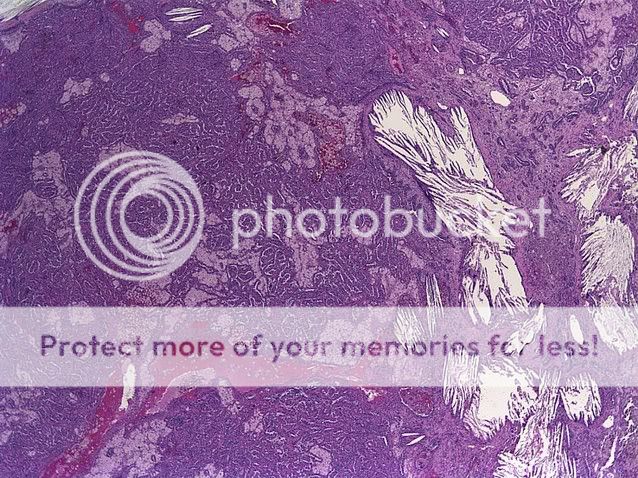
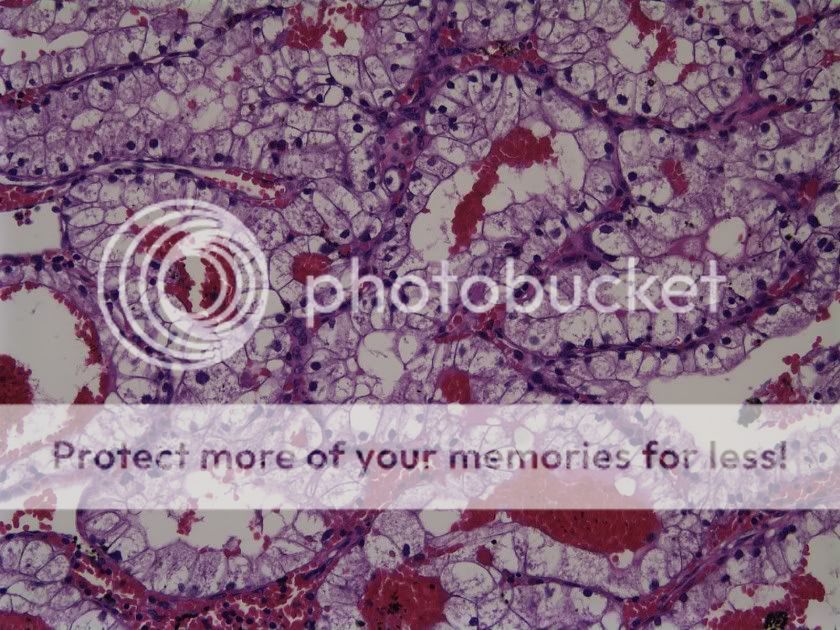
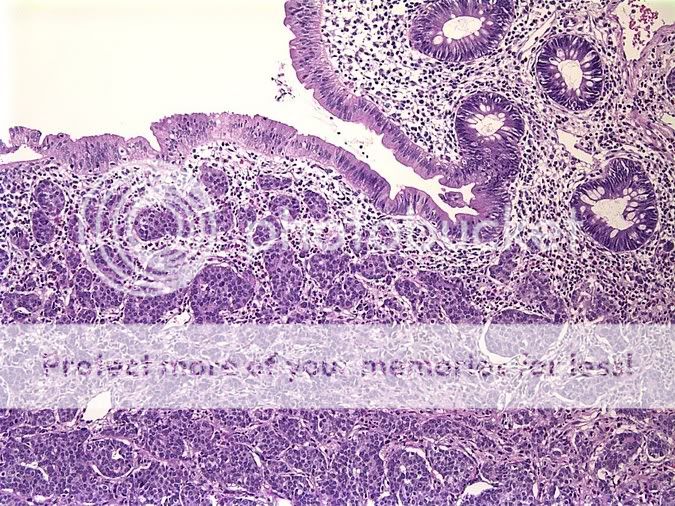
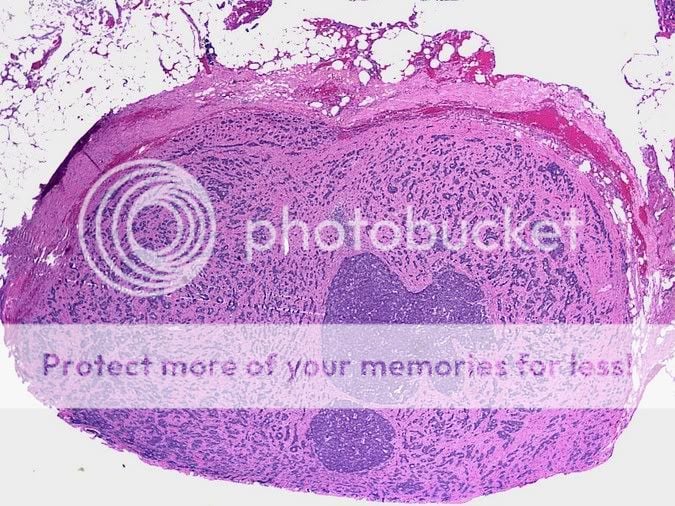
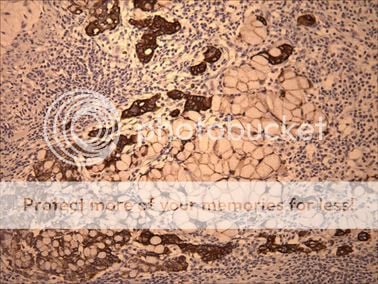
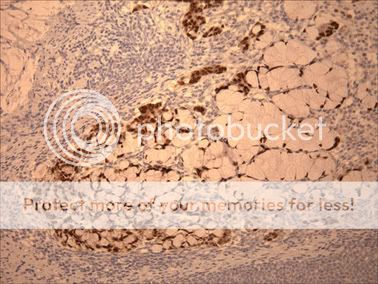
OK so the diagnosis on the first slide (beta-HCG above 200000)...complete hydatidiform mole. We saw big hydropic villi with cisterns and trophoblastic hyperplasia and atypical implantation sites. No fetal tissue identified microscopically (but in many products of conception slides, you don't see this) but not seeing fetal tissue on the slide in question further bolsters the diagnosis of complete mole.
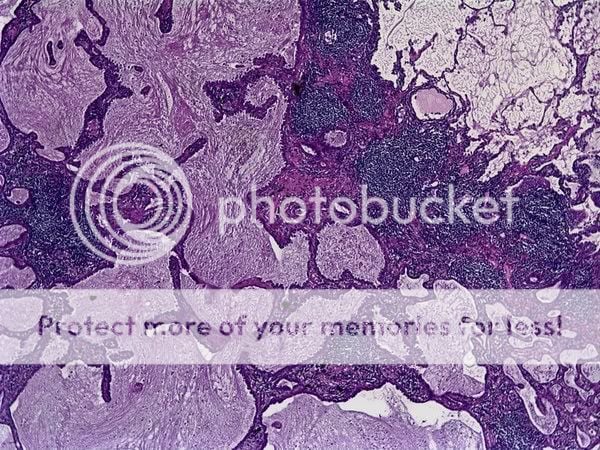
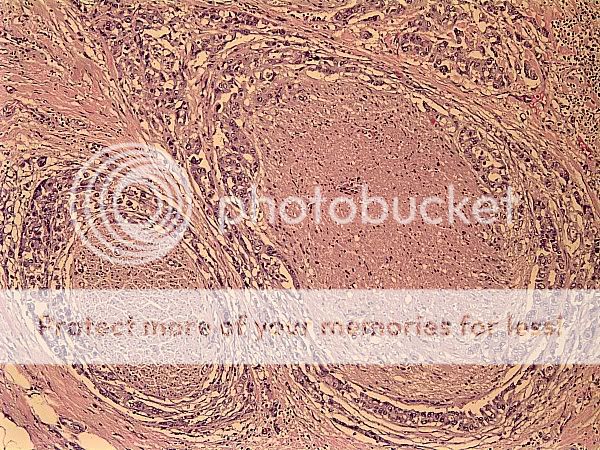
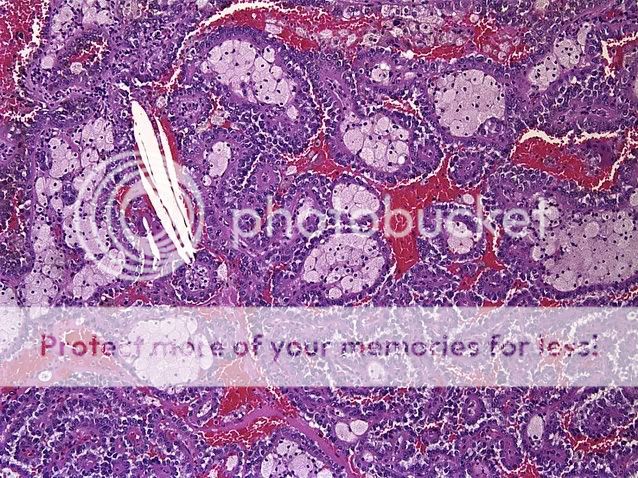
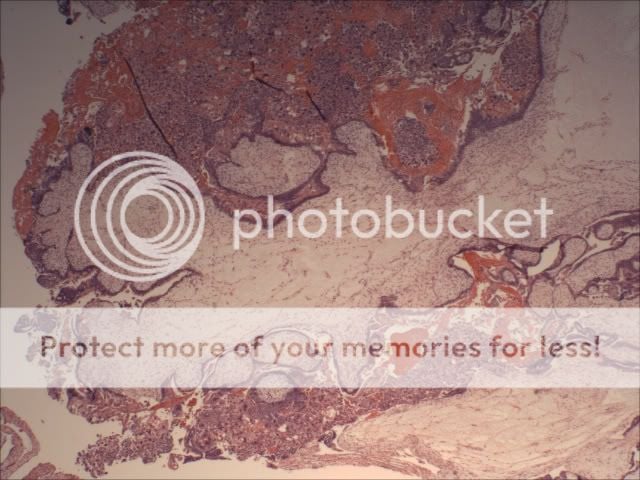
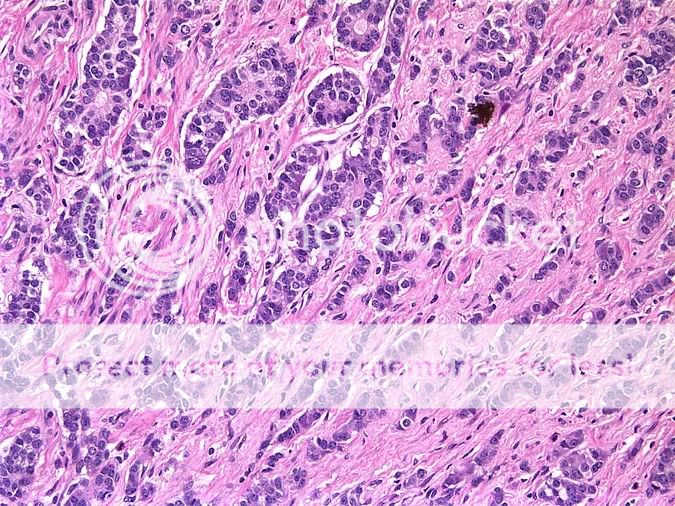
The second slide (previewed last night and in the process of being signed out) most likely represents an endometrial carcinoma (which is supported by the fact that she has a history of it! She gonna get her uterus taken out.) However, I saw a case where a papillary serous adenocarcinoma originating in an ovary was metastatic to the endometrium (usually, based on my limited experience, I'm used to seeing implants of metastatic papillary serous adenocarcinoma showing up on the serosal surface of the uterus, N=3). That case presented somewhat similarly to this one with a few differences that are outside the scope of this post. So just by looking at the slide, one could make a case for papillary serous. However, looking at the specimen in high power, the cancer looks more endometrioid. We're doing a p53 anyway to shed more light on the matter. We'll get the impox slide tomorrow and we should be able to sign it out soon thereafter.
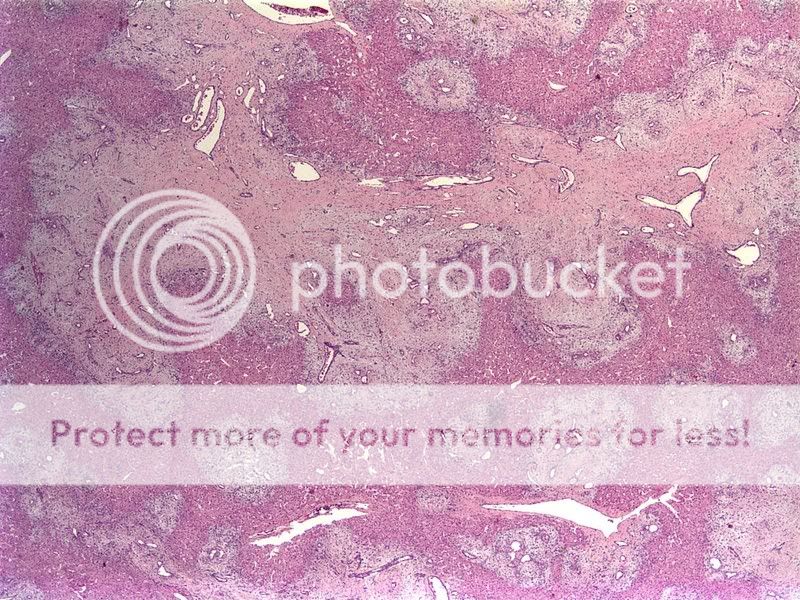
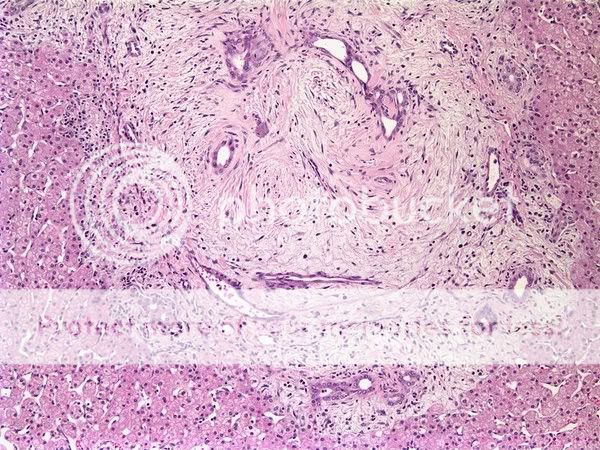
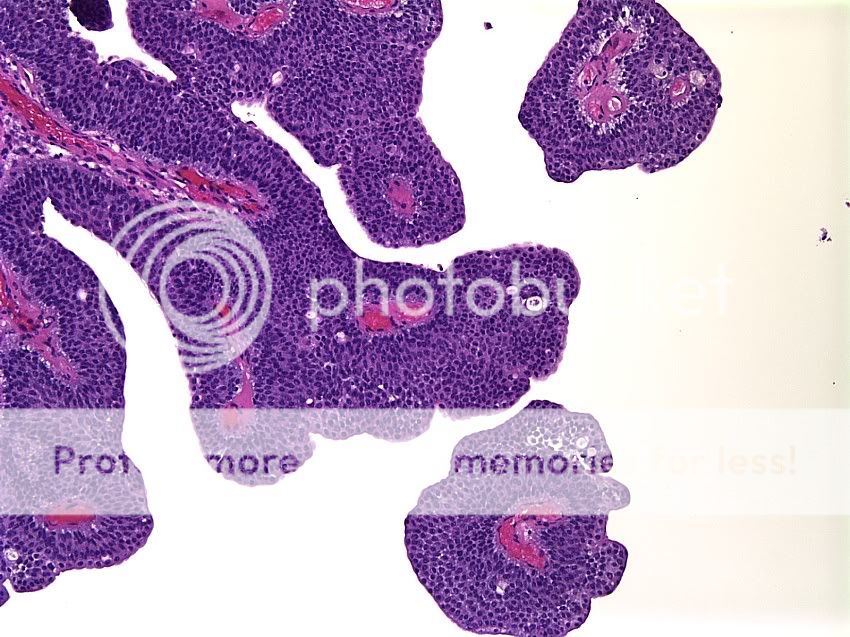
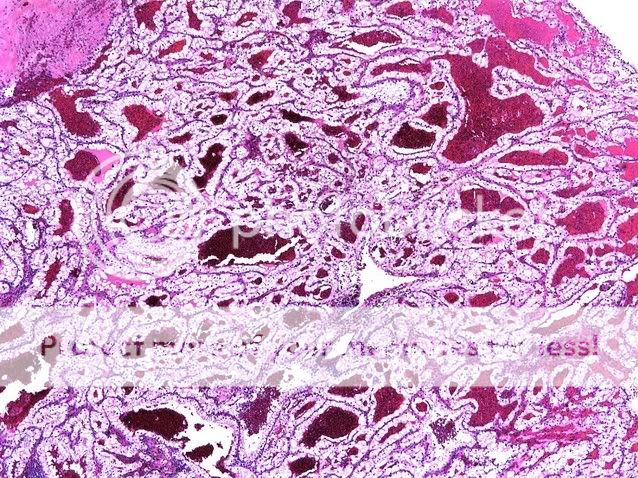
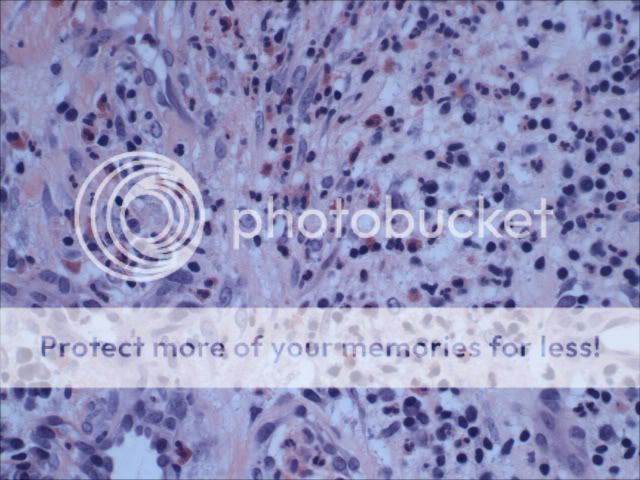
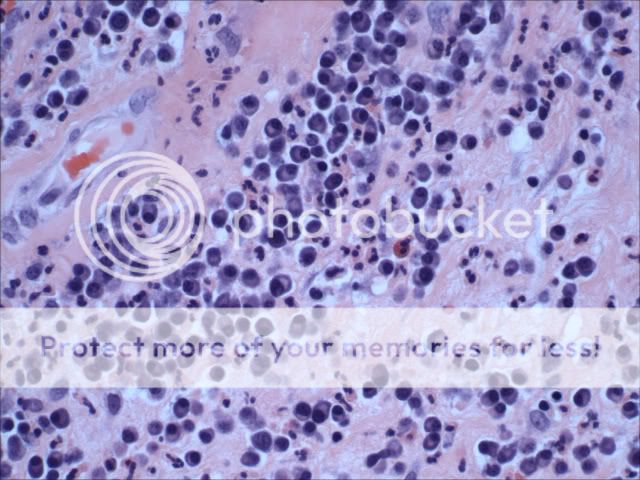
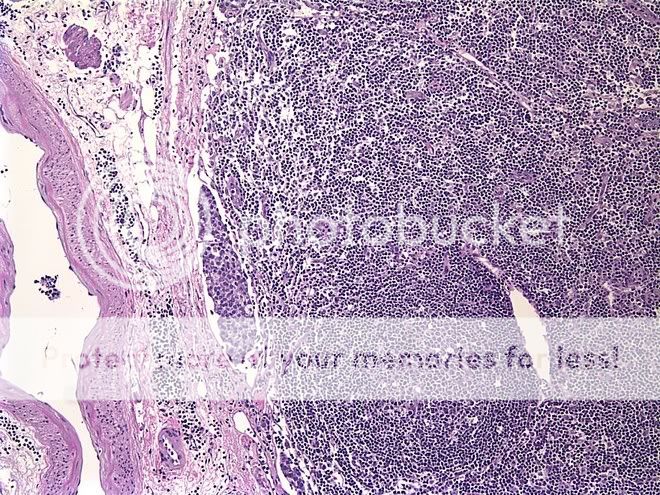
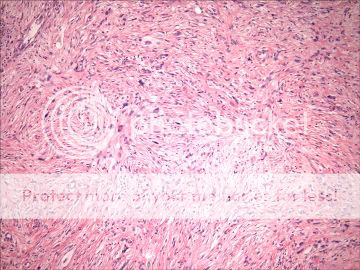
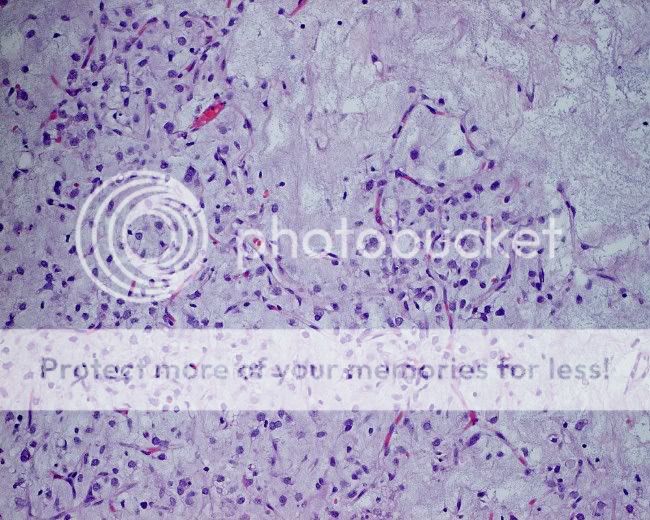
The third slide was sparked much confusion when I previewed it last night. Showed it to a couple of other residents and fellows. Could've been infectious given all that plasmacytic, eosinophilic, neutrophilic, yada yada yada infiltrate. However, at signout, it was called granulation tissue. Looked at the history this morning and the patient is status post hysterectomy. This specimen was taken from the apex of the vagina. Apparently, after these surgeries, patients can get these "cherry red" spots at the surgical scar. But this was a surprise to me nonetheless. But at signout it made sense as the attending was explaining it. If you look at the superficial aspect of the lesion, it does look like granulation tissue...and you can still get this kind of infiltrate. After all the mental masturbation that went on last night, the diagnosis is kind of a letdown. Still, a diagnosis has been reached and the case is signed out. Sayonara!