- Joined
- Apr 4, 2009
- Messages
- 17,237
- Reaction score
- 13,023
It's very, very hard not to bring your work problems home as a resident.As long as these antics don't come home, I'm okay with him being as drama queen as he likes")

It's very, very hard not to bring your work problems home as a resident.As long as these antics don't come home, I'm okay with him being as drama queen as he likes
It's very, very hard not to bring your work problems home as a resident.
Have your walls made of insulation. Those can be easily replaced.Meh, its okay. I was mostly kidding. We'll get through it
Have your walls made of insulation. Those can be easily replaced.
This is what I can't stand. A lot of things in that specialty are "unsaid" (hope that makes any sense). I mean it's not like you were standing there asking questions every 2 seconds ("Hey, is that the liver down there?" "Hey, is that where the cancer is where you're suctioning?") while the operating is happening with no social awareness. You were asking whether he needed another **** pair of hands to retract something.
You can't say anything all day, your BP increases, and then finally when you get home, you release your being pissed off by kicking the cat I guess.
I'm guessing Advanced Surgical Recall didn't have the answer. lol.
Identify the Portal Vein/SMV with Splenic vein posterior to the pancreas. Why? Because you usually identify those first when dissecting the back of the Pancreas. He wanted the IMV.Isolated SV thrombosis and it's sequelae Is what I think he was going for
Where's the away?
/continue rant
I mean,Wait, this is an audition rotation and this happened to you? Oh, good lord.
Yep. If they're trying to make me to NOT want to come here; congrats.No, I know that it won't go on the MSPE and no place will see it and he won't be getting an LOR (although the intent in doing it maybe was to get an interview there?) It's just that now it's relatively a waste of the month if he's banned off his cases and he's an evaluator (although hopefully not his main/only attending evaluator)
Although, maybe it's a blessing in disguise, because now he won't waste his time ranking a program that sounds pretty malignant. I would hate to have to deal with a personality like that for 5-7 years. Although there is a very good chance I will end up applying to gen surg, so it might be unavoidable.
Yeah,
At this point; I'm kind of "over" it. I'm just let down by the idea that I was interested in this program and this is what I've gotten out of it. I get I'm supposed to impress them, but this is a two way street. I'm not saying pave a red carpet, but give me a reason to want to come here instead of treating me like ****.
Read below:
Identify the Portal Vein/SMV with Splenic vein posterior to the pancreas. Why? Because you usually identify those first when dissecting the back of the Pancreas. He wanted the IMV.
I agree w/ SV thrombosis if you think "What are sequelae". But I couldn't ask him to clarify (It's a question - insta-ban).
I mean,
There are a couple good people. I'm just not interacting with them as much. The absolute most hilarious part was asking me on Friday to take 8 patients on the list and present them on Saturday rounds as part of my "evaluation". I pick the 8. We round as a group (3 teams, 40 patients - yeah, best time ever to have med student rounds with 3 residents post-call). We get to patient 1 and the attending is like "Oh, we don't round on those patients since that attending rounds by himself" I look at my list: My team has almost all patients with the one attending not rounding with us. There were 2 that were "presentable".
At that point... I didn't know what to think. I tried paging Ashton Kutcher. Because I don't know how I can pick 8 out of the 10 patients on the list and them not be presentable. I mean... you'd think someone would let me know that this attending doesn't round with the team.
Yep. If they're trying to make me to NOT want to come here; congrats.
It's not a blessing but an inconvenience/annoyance. I mean, long-term, it's convenient. Short term - I want to punch a wall like DermViser said.
Meh. There's a reason I don't study at my own place - I try to make a VERY sharp divide between my place and everything outside of it. When I get home - I don't study. I come back to my place and it's my sanctuary, so to speak. Yeah, I know it'll be damn hard not to do that 100%, but I'm working on it. I do know that having "my place" with it's setup like I want with the painted walls/decor does help.It's very, very hard not to bring your work problems home as a resident.
lolHave your walls made of insulation. Those can be easily replaced.
Can't ask questions in surgery? Why?
You know what happens when I ask one of our attendings a question they can't answer? They say they like working in academics because the residents keep them on their toes.
I wouldn't call it a temper tantrum necessarily, just being angry. You don't have to punch a wall. You could just throw things. LOL!!! Just replace them when you're done.I don't have that whole "temper tantrum with physical abuse" issue. I mean, a part of me wishes I was in Sons of Anarchy and I could be all Jax Teller with the throwing punches. But I know that physical actions never get you anywhere.
So after full surgery workday you plan on doing all your studying at the hospital and then come home?Meh. There's a reason I don't study at my own place - I try to make a VERY sharp divide between my place and everything outside of it. When I get home - I don't study. I come back to my place and it's my sanctuary, so to speak.
So after full surgery workday you plan on doing all your studying at the hospital and then come home?
I'm just surprised he'd still stay there after sign out and study. Most residents would want to just get the f home and study there.To dinner waiting for him, of course. And the princesses. And poms.
and a vesper martini.
Damn, I'm good.

I'm just surprised he'd still stay there after sign out and study. Most residents would want to just get the f home and study there.
Is the martini for u or him? Yum!
You're not living in an apartment?It's for him. They're too strong for me, I'm a lightweight, half of one and I'm stupid loopy and talking about unicorns. Also he's never studied at home, I like it that way. I know it's inevitable that there will be some spillover but when we're in a house and not a 2bdrm apt if he has work to do, he can go do it in his study.
Which will have a direct exit into the garage. With a shower. We are not tracking gross car grease into the rest of the house or anywhere near the princesses
You're not living in an apartment?
I just finished a TY surgical month:
1. The patients and problems are so much better than general IM, patients are usually younger and with fewer comorbidities. Making the diagnosis is not hard; deciding when to mobilize an OR team is.
2. You work a lot of hours, but your day is much busier. The surgeons here have straight up refused to use the **** EMR, so we are all paper-chart for admission/consult/progress notes and orders. We get a lot of **** done because we aren't hampered by Meditech (another rant for another thread).
3. God damn you work a lot of hours. I was pushing 90+ and this was on top of my commute (30 minutes each way). And when you're long call and a case is going at 6pm, you're staying to finish the case, no matter when it gets out. That led to a lot of staying until 9-10 pm. It was the irregularity that made it super tough; if cases are going, you don't get to leave at sign out.
4. If you LOVE operating (and I still do even though I'm going radiology), you'll put up with the absolute loss of control of your hours. If a patient needs an operation, you can't just sign it out to the night team. But I also basically didn't have a life for that month. My emails piled up. My mail piled up. My everything piled up.
5. Attendings make or break your rotation. I had 6 surgical attendings. 5 were great; 1 was a complete dingus and gave me **** about going into radiology every single time I operated with him (he would act like he would hand me a stitch, then say "if you were a real surgical intern, you'd be practicing knot tying every day" and then take the stitch himself). It got to the point where I asked my chief to assign me floor work over cases with him; luckily, my chief scheduled the other intern with that attending. As a comparison, the vascular attendings let me throw knots on their anastomoses. It's not like I don't know how to tie.
Our surgery months function like gensurg prelim months. Our medicine months are where it's at.You're doing TY all wrong.
I got so much traveling done during my surgical months. Picked up a few new hobbies too.
Agreed. But I'm just not like that. I have stages of angry:I wouldn't call it a temper tantrum necessarily, just being angry. You don't have to punch a wall. You could just throw things. LOL!!! Just replace them when you're done.
No, not hospital. There are other venues: Coffee shops, library, etc. My condo has a conference room that I also use when I "have to" study at my building. I just refuse to bring something as tiresome and depressing as studying at my place. If I do any sort of studying, it's light review/reading. Will it stay like this? I dunno. I just like to keep my place as a sanctuary.So after full surgery workday you plan on doing all your studying at the hospital and then come home?
I'm just surprised he'd still stay there after sign out and study. Most residents would want to just get the f home and study there.
Is the martini for u or him? Yum!
How can surgeons just outright refuse to use the EMR that the entire hospital uses?I just finished a TY surgical month:
2. You work a lot of hours, but your day is much busier. The surgeons here have straight up refused to use the **** EMR, so we are all paper-chart for admission/consult/progress notes and orders.
I forgot to ask (and this is where my paradox exists):
People keep telling me I need to show them how awesome I am which means outsmarting the residents. That seems like the worst idea ever... I don't want to disrespect or unintentionally insult the residents considering I'll be working with them...
I forgot to ask (and this is where my paradox exists):
People keep telling me I need to show them how awesome I am which means outsmarting the residents. That seems like the worst idea ever... I don't want to disrespect or unintentionally insult the residents considering I'll be working with them...
Damn that student was stupid.Take it from me. I'm getting killer evals. My psych preceptor is from an old generation that still regularly gives benzos to people with even mild clinical depression. And each time he tells his patients they need benzos for depression I just nod.
This is after I found out another student gave him an uptodate article on SSRI's and depression and that student got all 2's on his evals. He doesn't care to be corrected.
It's a community, low-income/safety-net hospital, so they need income any way they can get it. If they were to force the surgeons to use EMR, the surgeons will do their cases at the for-profit hospital across town. All surgeons, even ones in the physician's group affiliated with the hospital, maintain dual privileges just in case they get forced into using Meditech. All that OR, PACU, and inpatient billing to patients that actually have insurance will disappear (as elective surgical patients tend to have).How can surgeons just outright refuse to use the EMR that the entire hospital uses?
This is what happens when students are not taught the hidden curriculum by a sympathetic intern/resident/faculty member...Damn that student was stupid.
Ah, ok - that's what I figured. Didn't know how long that would last with Obamacare regulations saying that medical records must be in an EMR format.It's a community, low-income/safety-net hospital, so they need income any way they can get it. If they were to force the surgeons to use EMR, the surgeons will do their cases at the for-profit hospital across town. All surgeons, even ones in the physician's group affiliated with the hospital, maintain dual privileges just in case they get forced into using Meditech. All that OR, PACU, and inpatient billing to patients that actually have insurance will disappear (as elective surgical patients tend to have).
This is not the first hospital I have rotated at where surgeons have flat out refused to use the crappy ass EMR. I have posted pictures of this monstrosity to the forum previously. They get around meaningful use attestations by enrolling the surgeons in CPOE, but then they scan literally everything that is handwritten into a SEPARATE EMR silo so it can be attested to as "digital" or whatever.
I agree. There is a lot of hidden curriculum involved. I also think it's bc you have many students who have never worked a real job in their life before, and thus don't understand simple workplace norms and mores. This is something all your non-med school friends who went to work directly after college (engineering, etc.) figured out a long time ago. He could have easily asked the psychiatrist why he chose a benzodiazepine vs. an SSRI for depression and gotten his answer. Waving an UpToDate article in an attending's face, is not the right way to go about doing it.This is what happens when students are not taught the hidden curriculum by a sympathetic intern/resident/faculty member...
I thought nearly all hospitals used EPIC. That seems to be the go to EMR for all hospitals.i've seen your picture, i don't understand why anyone would spend money on that
i could probably make something better and it would only take a year
all these emrs look early 90s websites or they have tiny pages that make it impossible to find useful information
so far from the 5 or so i've seen, medent is the only one that isn't worthless
Only 40% marketshare.I thought nearly all hospitals used EPIC. That seems to be the go to EMR for all hospitals.
In other words, be a HAMMERHEAD: http://doctum-aphorism.tumblr.com/post/24552003854/the-perfect-surgery-studentAs a general surgery sub-I, you show people how awesome you are by how much s**t you can shovel for them so that they don't have to.
Talk to that discharge coordinator for them
Go bug the scheduler in radiology about getting the upper GI done in the morning instead of the afternoon
When the vitals for this shift haven't been recorded, track down the RN and get her to show you her handwritten records that she hasn't had time to type up yet
Make sure you know exactly how the chief likes his list printed (and how he likes his coffee to go along with it...only partially kidding)
Know every lab and vital on every patient so that when someone asks what the phos level was yesterday, you don't have to go fumbling around in the EMR for two minutes
etc.
etc.
And on top of that you need to know every bit of relevant anatomy and clinical knowledge of surgery.
That looks terrible. Looks like they bought the cheapest EMR they could get away with.Only 40% marketshare.
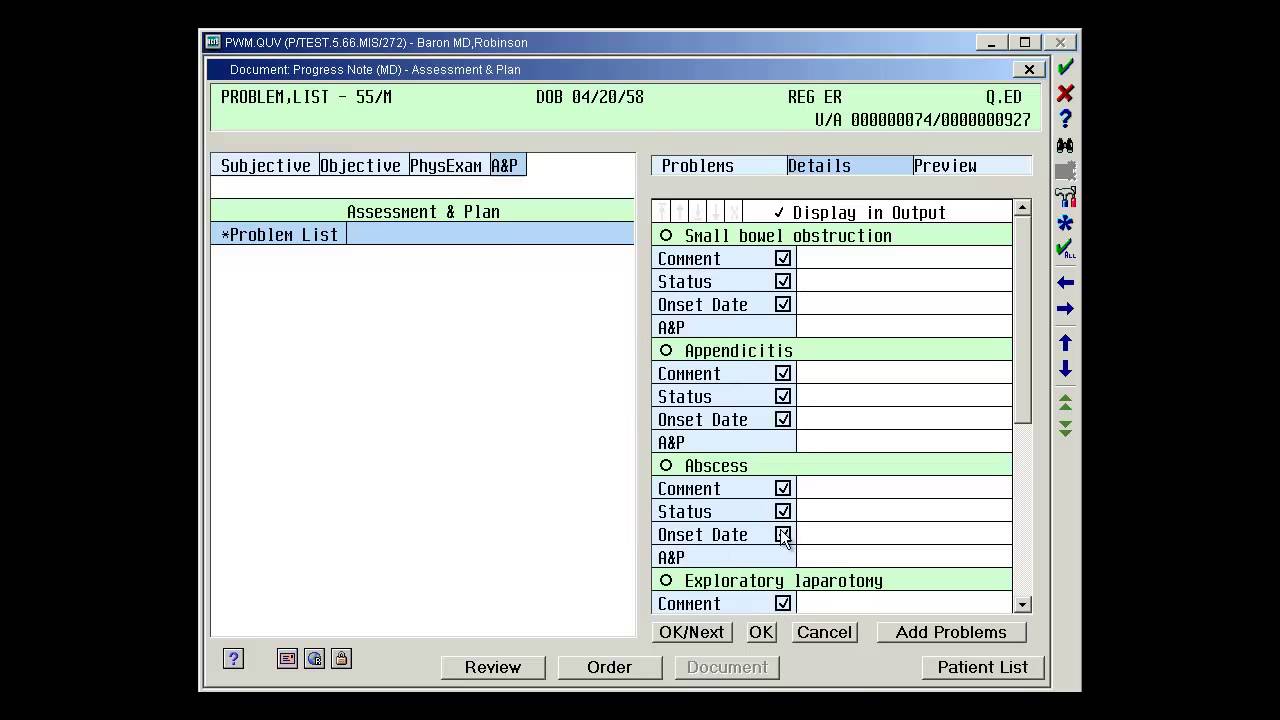
To those who haven't seen what I have to use daily, this is the POS I have to write progress notes with. Oh Meditech Magic, how I hate you.
The software dates to 1982.That looks terrible. Looks like they bought the cheapest EMR they could get away with.
And apparently made with MS-DOS.The software dates to 1982.
Outsmarting is the wrong word. I would call it more being on top of your game (yes, this can get exhausting). One can show how smart they are without being pompous or disrespectful to the team. I think you have to have some social awareness (not saying you don't) and gauge the situation. You don't want the label of overly aggressive, but not be labeled as aloof either.
YeahOh dear god no. "outsmarting the residents" is also a great way to get bad evals. You think they're going to be grateful for a medical student constantly correcting them/telling them how to work?
And apparently made with MS-DOS.
No, I understand being a little bit apprehensive. You're in a totally new place and getting thrown off would be jarring to anyone. Half the audition rotation is just getting acclimated. I think it depends how much that incident affects the others. No need to bring it up or keep apologizing - that makes it worse.Figured. I feel like I'm taking 3 steps backwards now after what happened last week. lol
I've played games in the early 90s that had a better interface
LOVED that video game. Gave me headaches though - so worth it.I'd play Wolfenstein 3D right now if I had the proper computer. Kill me some Hitler on a robot body.
LOVED that video game. Gave me headaches though - so worth it.
Only 40% marketshare.
To those who haven't seen what I have to use daily, this is the POS I have to write progress notes with. Oh Meditech Magic, how I hate you.
... the government's implementation is better.
The software dates to 1982.
Anesthesia residents definitely get crapped on by malignant surgeons. Just read some of the threads in the anesthesia forum.
You're going to be spending hours in a room with them at a time. Turns out you have to interact with the other side of the blood brain barrier pretty often.
Well first off, I reject the notion that all surgeons have malignant personalities. If that's all you've taken away from this thread, I don't know what to tell you.
My point was simply addressing your notion that as an anesthesia resident you wouldn't have to interact with surgeons. I don't know how you could have spent any time on an anesthesia rotation and come away with that impression.
As to why anesthesia residents are "happier" - I'd say first off that at my hospital my co-residents in anesthesia by and large aren't "happier" than my co-residents in surgery. But in general as a field and a training program? Probably because they are working on average 20 hours less per week.
But I'm not the best source to tell you all the positives and negatives of an anesthesia residency, since I didn't do one and never seriously considered it.