This
thread is an instructive snapshot of the
Revolution going on in lung cancer right now... and how rad onc is getting left behind. Its getting left behind is not in a Kevin McCallister-type sense but in the intellectual and cultural sense.
We have all felt this schism, yes? What is it that the medical oncologists and surgical oncologists see that the radiation oncologists don't. We are a bit "stuck." As you read through the thread, it is very much "
The Structure of Scientific Revolutions," one of the greatest books about science ever:
...Thomas Kuhn used the term ‘incommensurable’ to characterize the holistic nature of the changes that take place in a scientific revolution. His investigations into the history of science revealed a phenomena often now called ‘Kuhn loss’: Problems whose solution was vitally important to the older tradition may temporarily disappear, become obsolete or even unscientific. On the other hand, problems that had not even existed, or whose solution had been considered trivial, may gain extraordinary significance in the new tradition. Kuhn concluded that proponents of incommensurable theories have different conceptions of their discipline and different views about what counts as good science; and that these differences arise because of changes in the list of problems that a theory must resolve and a corresponding change in the standards for the admissibility of proposed solutions. So for example, Newton’s theory was initially widely rejected because it did not explain the attractive forces between matter, something required of any mechanics from the perspective of the proponents of Aristotle and Descartes’ theories. According to Kuhn, with the acceptance of Newton’s theory, this question was banished from science as illegitimate, only to re-emerge with the solution offered by general relativity. He concluded that scientific revolutions alter the very definition of science itself.
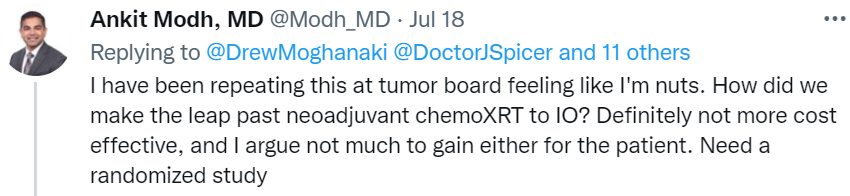
Also, Drew M got pwned (this happens when you're operating outside the revolution vs within it, or affecting it):