- Joined
- Jan 24, 2014
- Messages
- 1,362
- Reaction score
- 2,944
could you use lack of overhead as leverage to ask for a higher percentage of inpatient work?
Absolutely.
The only problem is that greedy private practice owners won't agree to it.
could you use lack of overhead as leverage to ask for a higher percentage of inpatient work?
Yeah but you got that inpatient consult based on the goodwill of your employer. That is emotional overheadHas anyone heard of, or had any luck, negotiating a higher percentage for any inpatient work they do in the hospital outside of PP, given that hospital work has no overhead for the owner? Essentially, since there’s no overhead for inpatient work, could you use lack of overhead as leverage to ask for a higher percentage of inpatient work?
Emotional overhead CRUSHES associates. That and owners' wives...Yeah but you got that inpatient consult based on the goodwill of your employer. That is emotional overhead
Hospital work doesn't pay much anyway. Hospital patients does not really pay well because you have the self pay (no insurance) patients, $20k deductible insurance, medicaid patients, measly medicare etc. Once in a yellow moon you will have the holy grail private insurance (BCBS, Cigna, Aetna etc) that pays you like a real doctor. As I said in my previous posts, you can't build your practice or income on taking FREE hospital ER call or doing inpatient consult work. Those are charity work.Has anyone heard of, or had any luck, negotiating a higher percentage for any inpatient work they do in the hospital outside of PP, given that hospital work has no overhead for the owner? Essentially, since there’s no overhead for inpatient work, could you use lack of overhead as leverage to ask for a higher percentage of inpatient work?
Well my friend, right now it’s not really up to me. It’s part of my job so I’m doing it. There have been some uninsured patients, yes, but luckily to this point they haven’t required a ton of work on my behalf. There has also been a nec fasc patient whose limb I was able to salvage and luckily insurance has paid pretty well for. Hopefully it evens out? So I’m just thinking in the future of what I can do to make that aspect of my work more worth my time.Hospital work doesn't pay much anyway. Hospital patients does not really pay well because you have the self pay (no insurance) patients, $20k deductible insurance, medicaid patients, measly medicare etc. Once in a yellow moon you will have the holy grail private insurance (BCBS, Cigna, Aetna etc) that pays you like a real doctor. As I said in my previous posts, you can't build your practice or income on taking FREE hospital ER call or doing inpatient consult work. Those are charity work.
Also forget those who say you "build your name" by taking FREE hospital call or consult. You can't make much revenue from self pay (no insurance) patients or medicaid patients. These are the frequent flyers at the hospital. Let the hospital employed folks deal with it.
Sounds like the attending is employed by the MSG and subcontracting you out...A few things to ask about an offer being drafted by a MSG with one of my attendings:
- 1099 paying 110k + 35% gross at 315k
- Even as 1099 there was mention of providing health/malpractice/401k which I don't understand.
- There's also inpatient work, wound care centers which they didn't clarify how it's paid out yet. I would hope it's separate from the 35% considering it's not associated with their group.
- Isn't being paid a % of collections as 1099 a violation of anti-kickback? Or does that only apply to net, not gross collections?
You seem to be receiving a private practice offer but with questionable tax dynamics. How many days a week will you be working for the MSG?A few things to ask about an offer being drafted by a MSG with one of my attendings:
- 1099 paying 110k + 35% gross at 315k
- Even as 1099 there was mention of providing health/malpractice/401k which I don't understand.
- There's also inpatient work, wound care centers which they didn't clarify how it's paid out yet. I would hope it's separate from the 35% considering it's not associated with their group.
- Isn't being paid a % of collections as 1099 a violation of anti-kickback? Or does that only apply to net, not gross collections?
A few things to ask about an offer being drafted by a MSG with one of my attendings:
- 1099 paying 110k + 35% gross at 315k
- Even as 1099 there was mention of providing health/malpractice/401k which I don't understand.
- There's also inpatient work, wound care centers which they didn't clarify how it's paid out yet. I would hope it's separate from the 35% considering it's not associated with their group.
- Isn't being paid a % of collections as 1099 a violation of anti-kickback? Or does that only apply to net, not gross collections?
Sounds like the attending is employed by the MSG and subcontracting you out...
1. I think we both know a person who works for the same business 5 days a week is really an employee and not an independent contractor. This may or may not be something the government comes after in the future. My suspicion is the government is more interested in protecting low income employees but we'll see.Nothing is really drawing me to it, just gathering whatever offers I can get. It's 5 days per week. Apparently every physician is employed as 1099, including this attending. The dynamics make no sense to me. How can you be 1099, with benefits, without any sort of additional hidden structure?
I don't understand the dynamic of essentially a W2 structure but 1099? This is the first time I hearing of a 1099 position in Podiatry and wasn't told about it ahead of time, so I didn't know what questions to ask. Really just trying to get info about this sort of structure in case it comes up again. I don't have any draw or reason to this specific offer if it's bad.
Merry Christmas everyone!
Long time reader here. Finally decided to make an account and maybe contribute a thing or two.
As someone who is currently in the job market, I can say that everything posted on this forum is extremely accurate. For those who say there are numerous good jobs posted, you’re crazy. The market sucks. There are very few MSG, hospital or ortho jobs available. With that being said, I was just offered a job and wanted to ask a question about call to those who are in MSG or hospital groups. How much call are you guys taking or required to take? Due to the set up of this particular job, I would have to be on call 1:2, which feels like a ton. And no, it is not in the most desirable area. Even if the call isn’t busy, I feel like having to be available this much makes it feel like you don’t have much freedom.
Appreciate all input!
Merry Christmas everyone!
Long time reader here. Finally decided to make an account and maybe contribute a thing or two.
As someone who is currently in the job market, I can say that everything posted on this forum is extremely accurate. For those who say there are numerous good jobs posted, you’re crazy. The market sucks. There are very few MSG, hospital or ortho jobs available. With that being said, I was just offered a job and wanted to ask a question about call to those who are in MSG or hospital groups. How much call are you guys taking or required to take? Due to the set up of this particular job, I would have to be on call 1:2, which feels like a ton. And no, it is not in the most desirable area. Even if the call isn’t busy, I feel like having to be available this much makes it feel like you don’t have much freedom.
Appreciate all input!
10 days is pretty standard. Even if MSG may not require it in a contract, most hospitals where you will have surgical privileges will require it.10 days per month. Unpaid, but I’m employed so I’m guaranteed to get paid for the work I do on call. Also not busy at all, rarely get called in. But the problem with being on call every other week is the inability to get too far away from the hospital.
I would attempt to negotiate that to something more reasonable, even if you are going to get paid daily to be on call.
Whoa whoa whoa slow down here...this is crazy talk. I know lots of grads from big university programs that have no problem finding private practice jobs.Merry Christmas everyone!
Long time reader here. Finally decided to make an account and maybe contribute a thing or two.
As someone who is currently in the job market, I can say that everything posted on this forum is extremely accurate. For those who say there are numerous good jobs posted, you’re crazy. The market sucks. There are very few MSG, hospital or ortho jobs available. With that being said, I was just offered a job and wanted to ask a question about call to those who are in MSG or hospital groups. How much call are you guys taking or required to take? Due to the set up of this particular job, I would have to be on call 1:2, which feels like a ton. And no, it is not in the most desirable area. Even if the call isn’t busy, I feel like having to be available this much makes it feel like you don’t have much freedom.
Appreciate all input!
It's important to distinguish: are you meaning 1 on call : 2 days off (ratio, as you posted)... or 1-in-2 (every other week... half of total)? Huge difference. Jobs, especially MDs, usually state the call as being "1-in-X" or the "qX" (every X days) way, so I'm guessing you do mean the latter, q2 or 1-in-2?...Due to the set up of this particular job, I would have to be on call 1:2, which feels like a ton. ...
Sorry let me be more specific. It is 15 days a month, split into 3-4 days/ week depending on the week. Guaranteed 2 weekends per month. If I wanna get on the trauma call rotation, that’s another 6-7 days per month. Those can be stacked where I would be on both calls at the same time, but there’s like our a few days where it doesn’t work that way. So I’d be looking at 15 to probably 17 or 18 days per month.It's important to distinguish: are you meaning 1 on call : 2 days off (ratio, as you posted)... or 1-in-2 (every other week... half of total)? Huge difference. Jobs, especially MDs, usually state the call as being "1-in-X" or the "qX" (every X days) way, so I'm guessing you do mean the latter, q2 or 1-in-2?
Standard at most hospital jobs I have ever looked at is 1-in-3 or q3. The format may vary, but you are usually on the hook every third day/week/weekend on average... however they split it up. I have seen as high as half the days (1on:1off) aka 1st-15th of each month, etc at places where there is no other DPM on staff or only one other DPM or no other who is qualified/willing to take call. This is unfortunately not uncommon.
There are the rare jobs where podiatry doesn't take call, but they are the tiny minority of any DPM hospital jobs anymore... perhaps certain ones in places that have an extremely hard time attracting or keeping a DPM or docs of any kind. I have run across those docs, but they're typically ones who have been there decades and basically just do clinic and wounds and have no surgical training - never new job postings.
The most problematic thing to realize with call (outside that it's lame) is that the call can change. That is almost more key to remember than the fact that it's good/bad to begin with. If a senior DPM who takes call leaves or decides they won't take call any more, will you be on call much more? If someone is hired later, will you go from q3 to q4... or will a senior person just stop taking call. You need those things IN WRITING... max call days per month, max call days per year, HUUUUGE financial incentives or right of refusal for you if you are pushed to take more call than agreed.
This part of it is the main reason I don't think I'd look seriously at a hospital job with requisite call again (or a PP pod/ortho/MSG one either). It is just too much on your QOL... I've found that I much prefer taking call on my own pts or when I can, but it's always optional and I never have to loathe phone calls. It's just what's better for me and my sleep, my health, and my personal life (and probably my stress level is better for hospital and office co-workers!).
...And yes, as @bloxxeeey alluded, those are your basic 5 or 6 job options as a DPM:
- PP small group... low pay, bonus hit or miss, usually hours ok, sometimes decent partner/buyout path
- PP large group... salary higher but must produce high pt vol and/or do shady stuff to hit bonus, almost zero chance partner/owner
- hospital employ... competitive to get/keep jobs, higher end pay, on-call, politics/admin pressures
- MSG/ortho.. highly variable... usually elements of both large pod PP and elements of hospital
- owner/solo... hard to start, many places are tough to get refers and find cases for boards, ok for some DPMs esp rural
- NH and/or house calls... tough work, ok pay at some, pressure to do creative coding, not using your skills
How much do they expect you to come in? What do they expect your numbers to be? Obviously if production is easy to get them you don't care about 230k to go away, but it's still nice to have an underlying base. Are they desperate for another pod? If not then you want a 2 year guarantee. That is a lot of call. I don't know of pods taking that much. I don't know many other specialties taking that much without significant compensation. Like rural general surgeons.Sorry let me be more specific. It is 15 days a month, split into 3-4 days/ week depending on the week. Guaranteed 2 weekends per month. If I wanna get on the trauma call rotation, that’s another 6-7 days per month. Those can be stacked where I would be on both calls at the same time, but there’s like our a few days where it doesn’t work that way. So I’d be looking at 15 to probably 17 or 18 days per month.
It is not a bad offer financially speaking. $230k one year guarantee unless I exceed in collections, $25k signing bonus and $15k moving stipend.
I’m struggling most with my freedom and QOL. It is not an area that my family lives, and I feel that much time having to be around would make it tough for my family and I to travel or get away.
It wouldn’t be uneven call. One of the current guys is retiring when whoever comes in next starts, so there will be two total, hence the 15 days of call per month. Either way, it’s a lot in my opinion.Uneven call should always be a major dealbreaker. At some point groups get filled up with older DPM that feel they are better than call and dump it on the young. I had to tell my boss at one point flat out "I'm not taking your week because I dont have to" based on my contract.
Sorry but I hate inpatient work as a PP doc, especially when there are many hospitals to cover within a group. Nothing ruins my mood faster than a list of "global patients" then a call for uninsured patient that the ER doc wants us "to lay eyes on"
It is still a very good job compared to PP. This job stability and income potential both seem good.It wouldn’t be uneven call. One of the current guys is retiring when whoever comes in next starts, so there will be two total, hence the 15 days of call per month. Either way, it’s a lot in my opinion.
And I totally agree on taking call as a PP doc. This is a large multi specialty group but functions like a private practice essentially. The only upside is that most of the people there are insured as it’s a small-ish town and there are a few major employers that most people work for, so the amount of uninsured is very very low. They showed me the breakdown and I was actually surprised how low it was.
For me it’s mostly that I would have to be available basically half of the year at minimum. And trying to figure out how much $$ that call time is worth to me if I were to turn down and take a potentially lower paying job with less call.
Yeah I totally agree. Compared to PP it is a very good job. And honestly I think it’s a good job in general, just not ideal location for us currently.It is still a very good job compared to PP. This job stability and income potential both seem good.
If you have generous vacation that goes a long way. 6 weeks of vacation and the ability to also be able to afford to pay for relatives flights to come visit goes a long ways. It is never the same as being close for help with childcare, relationships of children with family and helping care for a sick parent etc. If you are married does you spouse have a flexible or a job where they can work remotel?
For me it would come down to what is my next best offer closer to where you want to be. Are there expensive buy ins to become a partner and if so what is the process to buy back your shares if you leave.
If you are unhappy there after a few years, but are busy and become board certified by ABFAS, it is never guaranteed, but you stand a good chance to find a good job closer to home if that is what you find you really still want.
Much appreciated. It has come with tons of effort, way more than one should have to put in for a “good” job, in my opinion.First and foremost congratulations on getting the job offer and an upcoming interview. Good organizational jobs, unfortunately too often come with some geographic compromise.
No easy answer on the stall. Some have lost jobs by stalling too long. You might be able to stall 3 weeks, especially with the holidays, but there is no telling how quickly things would move with the other hospital if you are their top candidate before you have an offer in hand. Most often the current offer would give you a hard deadline if they think you are taking too long before rescinding, but you never know for sure.
I would keep things vague and not be direct about the other interview.
Good luck figuring things out. It sounds like they really want you at that job. If they said they would give you time, they probably will. They would most likely say when they feel they have waited long enough we need to know by end of week etc before rescinding offer.Much appreciated. It has come with tons of effort, way more than one should have to put in for a “good” job, in my opinion.
They actually didn’t give me a hard deadline. And I straight up asked them. They said it’s not their way of doing things, but they also don’t want to wait around forever. I think that’s completely fair. I don’t plan on jacking them around, but I really wanna see what I think of this next place. I’m kind of at the point that I feel I need to be ready to walk away/they rescind the offer due to the time I need to stall.
The current offer comes with the amount of call we’ve talked about, plus a flight away from our families. Not the end of the world, but definitely makes a difference when it comes to kids, being around for holidays, family birthdays and things like that. This is also assuming I’d even get the next offer, and how long it would take for that to even come to fruition. I have found myself stressing over this situation a lot the last week and it helps getting opinions on here.
Good advice above. I would lean to taking the job unless you or spouse/partner abhors the area, just doing the call, getting your numbers for board cert ABFAS, smashing down your loans. Never bank on the "will be retiring" and "when you partner" stuff... get it in writing if you are hinging your plan on any of that... and still don't assume it will all happen exactly that way you were told at your interview visit.Yeah I totally agree. Compared to PP it is a very good job. And honestly I think it’s a good job in general, just not ideal location for us currently...
")
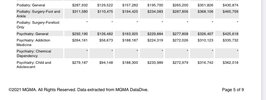
These numbers are higher than I figured. I feel like most hospital/MSG/ortho offers are lower than median MGMA, yet they say they go off of MGMA. Do you guys think there’s value in using this when negotiating pay? Of course, the big issue is that there’s always someone willing to take less in podiatry.2021 MGMA data for those wondering.
Mean comp in first column, median comp 3rd from left.
Oh yeah totally you should use. The question is how to get the info without paying for it...These numbers are higher than I figured. I feel like most hospital/MSG/ortho offers are lower than median MGMA, yet they say they go off of MGMA. Do you guys think there’s value in using this when negotiating pay? Of course, the big issue is that there’s always someone willing to take less in podiatry.
Happy NYE everyone!
Oh yeah totally you should use. The question is how to get the info without paying for it...
There is also AGMA and a 3rd one. I had one job that used an average of all 3
How do you get the info?Oh yeah totally you should use. The question is how to get the info without paying for it...
There is also AGMA and a 3rd one. I had one job that used an average of all 3
You can pay for it I believe maybe 6 or 7 hundred? It's expensive. But if you can call them out and say yeah um no that is not 50th percentile.How do you get the info?
My most recent offer said they use MGMA, yet the offer is $50k below what’s listed there as median for even general podiatry. Funny how that works
My most recent offer said they use MGMA, yet the offer is $50k below what’s listed there as median for even general podiatry. Funny how that works
I knew they did regional subdivisions of MGMA but I didnt know MGMA included benefits and 401k. I looked it up and according to Google (and Dtrack)MGMA numbers are “compensation” and include some benefits (ie signing bonus, student loan repayment, 401k match stuff, etc.) as well as production pay/bonuses above base salary.
Also, MGMA data the hospital uses is going to be region specific. MGMA publishes that data but the free sources that post this stuff usually don’t include it. Which means the national average seen in many of these spreadsheets and screenshots are going to be higher than what people in much of the “south” region are offered, for example.but they may also be lower that what people get offered in higher paying regions.
A base salary of $250k doesn’t mean you aren’t getting median MGMA “compensation”
Congrats, broski. Solid offer.Got (and accepted!) this offer. Working on contract negotiation but probably won't be much because it's a big hospital system.
Private practice group part of a large university healthcare network
Base is $150k
Bonus 10% after 400k
Partnership after 5th year with no buy in or other stipulations (partners all making $500k+)
Will be filling in the spot of a retiring partner so hope to be busy pretty quickly
No hospital call
All CME, malpractice, overhead covered
Larger, mostly suburban city
It's basically my dream setup in our number one area to live so overall couldn't be more excited. I wish the bonus structure was better (and I've wrestled a lot with it) but there's no buy in to make partner so I'm just trying to focus on the long term reward. Decent pay/base right out the gate but I feel like I'll be wishing for more growth in years 3-5. Good chance for me to have a solid initial contract and prove my worth I guess.
Bill a million in collections and make $210k (base + 10% of 600k)? Yikes. Maybe I’m missing something, but I fail to see the reason for such excitement. Someone with a straight 20% gig that bills a million would make the same, and that’s not a good offer.Got (and accepted!) this offer. Working on contract negotiation but probably won't be much because it's a big hospital system.
Private practice group part of a large university healthcare network
Base is $150k
Bonus 10% after 400k
Partnership after 5th year with no buy in or other stipulations (partners all making $500k+)
Will be filling in the spot of a retiring partner so hope to be busy pretty quickly
No hospital call
All CME, malpractice, overhead covered
Larger, mostly suburban city
It's basically my dream setup in our number one area to live so overall couldn't be more excited. I wish the bonus structure was better (and I've wrestled a lot with it) but there's no buy in to make partner so I'm just trying to focus on the long term reward. Decent pay/base right out the gate but I feel like I'll be wishing for more growth in years 3-5. Good chance for me to have a solid initial contract and prove my worth I guess.
Agree. And a LOT can happen in 5 years.Bill a million in collections and make $210k (base + 10% of 600k)? Yikes. Maybe I’m missing something, but I fail to see the reason for such excitement. Someone with a straight 20% gig that bills a million would make the same, and that’s not a good offer.
I'm a little unclear how it is both private practice and a hospital network. Let's ignore the salary and "bonus" for a second. If this was on the MD forums and the afforementioned salary/bonus was appropriate - people would still cringe at this in every way because 5 years is a long time. The first question asked would be - what percentage of people make it to partner, how many people have made it etc. Additionally, if you aren't paying for partner with a buy in then you are paying for it with sweat. How many associates does this group have? Is the partner money a reflection of skimming off the associates? What are the partner sources of revenue ie. is that because their collections are so high or because they own ...imaging, surgery center, etc.Got (and accepted!) this offer. Working on contract negotiation but probably won't be much because it's a big hospital system.
Private practice group part of a large university healthcare network
Base is $150k
Bonus 10% after 400k
Partnership after 5th year with no buy in or other stipulations (partners all making $500k+)
Will be filling in the spot of a retiring partner so hope to be busy pretty quickly
No hospital call
All CME, malpractice, overhead covered
Larger, mostly suburban city
It's basically my dream setup in our number one area to live so overall couldn't be more excited. I wish the bonus structure was better (and I've wrestled a lot with it) but there's no buy in to make partner so I'm just trying to focus on the long term reward. Decent pay/base right out the gate but I feel like I'll be wishing for more growth in years 3-5. Good chance for me to have a solid initial contract and prove my worth I guess.
I would guess that the other partners are making 500k (if that’s even true) partially because they’re making ~40% off their new associate’s collections.Agree. And a LOT can happen in 5 years.
YuckBonus 10% after 400k
Not really decent pay. If you collect $600k (a reasonable number if you’re really stepping into a full clinic) you make $170k. There is zero incentive for you to do more than $400k worth of work for the first 5 years.Decent pay/base right out the gate but I feel like I'll be wishing for more growth in years 3-5.
It was a private group for a long time that was purchased by the university healthcare system. They are now under the umbrella of the system and have all the resources, but still have all the say and control like in the practice (for example I didn't meet with anyone from "corporate," the docs were the ones who had the say in bringing me on). Maybe there's a better way to say it but it feels like sort of a mix of private and hospital based.I'm a little unclear how it is both private practice and a hospital network. Let's ignore the salary and "bonus" for a second. If this was on the MD forums and the afforementioned salary/bonus was appropriate - people would still cringe at this in every way because 5 years is a long time. The first question asked would be - what percentage of people make it to partner, how many people have made it etc. Additionally, if you aren't paying for partner with a buy in then you are paying for it with sweat. How many associates does this group have? Is the partner money a reflection of skimming off the associates? What are the partner sources of revenue ie. is that because their collections are so high or because they own ...imaging, surgery center, etc.
I'm happy that you're happy, but the financials and dynamics of this group are perplexing and its hard to imagine a circumstance where a person should receive such a poor bonus as their collections increase. What would you say if you found out you had $600K collections a few years in a row and the group ultimately told you that you'd paid more than a million dollars in sweat equtiy. Would that seem fair to you?
It was a private group for a long time that was purchased by the university healthcare system. They are now under the umbrella of the system and have all the resources, but still have all the say and control like in the practice (for example I didn't meet with anyone from "corporate," the docs were the ones who had the say in bringing me on). Maybe there's a better way to say it but it feels like sort of a mix of private and hospital based.
Group is 4 partners (one retiring) and 2 associates (both grads within the last couple years). They've only had one guy leave the practice and he was a partner (and he went to a group in another area if I remember correctly.
Obviously I'm not oblivious to the fact that it's really a bad bonus structure. I'm not banking on it but I do believe there will be some opportunity for renegotiation in the future.
Note- I haven't signed with them yet but contract is in the works so I do appreciate the input and maybe there will be some leeway for a better bonus.
The only thing that really matters is you like the job and the area. But don’t kid yourself, the contract is not good and 5 years to partner (even with no buy in which isn’t uncommon in MSGs) is way too long. 3 years of underpaid labor should be more than enough for you to be able to eat what you kill
Can you negotiate a shorter time frame to be partner? My partnership track in my MSG is 2 years. 5 is awful long. Do you know the numbers of the partners? Maybe reach out to the retired partner and get their honest feedback.