- Joined
- Mar 21, 2013
- Messages
- 1,934
- Reaction score
- 2,086
Good point depends on the individualDepends on the individual....but 5 years would be nice.

Good point depends on the individualDepends on the individual....but 5 years would be nice.
Good point depends on the individual
Handshake? I prefer the dead fish.you said you wanted to have surgery somewhere that could guarantee you an experienced anesthesiologist. If it depends on the individual, how would you determine preoperatively if they were acceptably experienced?
No one else in the room noticed the sudden silence of the pulse OX? He or she didn't notice the pulse is wasn't picking up? Or the lack of ETCO2?I bet an overwhelming majority of people would choose having an anesthesiologist over an independent CRNA if given a choice. My parents are not doctor people at all, and they get spooked by stories passed on by their church friends. I actually just had this conversation with my mom over the phone yesterday, seriously...
Mom: so I have a friend of a friend whose brother's wife is an anesthesiologist
Me: uh huh ok
Mom: and she was taking care of uh... 2 to 3 patients in an operating room? I've never heard of this... why would they put 2 to 3 patients in the same room?
Me: she was probably supervising 2 to 3 operating rooms. Each room has one patient, and the anesthesiologist goes around to each room checking on them during surgery. This is common.
Mom: oh ok that makes sense... and there was a nurse practitioner? helping the anesthesiologist?
Me: a certified registered nurse anesthetist
Mom: a what?
Me: *explains for 2 minutes*
Mom: oh ok, so the nurse saw that the patient's heart stopped beating on the EKG, and she just thought the machine wires stopped working
Me: EKG leads fall off a lot. that happens frequently
Mom: no but, the patient's heart actually stopped beating! and the nurse didn't call in the anesthesiologist for a long time because she thought it was an EKG problem
Me: what.
Mom: so the patient died, and the patient's family is suing the anesthesiologist and the nurse
Me: that makes no sense mom--what--how--wouldn't they see--
Mom: that's so scary! how is this allowed to happen? why can't the anesthesiologist be in the room the entire time???
If I'm a fellow anesthesiologist, or perhaps other physician, then presumably I would already know or could ask.you said you wanted to have surgery somewhere that could guarantee you an experienced anesthesiologist. If it depends on the individual, how would you determine preoperatively if they were acceptably experienced?


Obviously anesthesia has less documentation and less patient contact (at least when they're awake). That's not the point of contention here. The discussion is the tenuous future of anesthesiology and how that will affect your career in the next 20-30 years. Not having patient contact obviously has its upside, but it makes you more readily replaceable, especially when you've been training your replacement for decades. Ownership of patients may not provide complete protection from encroachment, but it's enough for now... whether or not that is worth patient contact is up to you.Little to no documentation with EMRs intra-op, watching ESPN and drinking scotch after the last days case sums up what most of the Attendings here do every night they're not on call. IM rounding, lecturing pts and nurses, social work etc. left me wiped out by the end of the day. The fast pace (PP not academic) and minimal pt interaction in Anesthesia is hard to replicate in IM unless youre scoping or stenting each day with occasional call and no clinic/rounding responsibilities, which I'm sure is possible.
Lots of gloom and doom on this thread. The fact is that we cannot predict what the future holds. I think there is a lot of fear of the unknown here. Fight for your livelihood, but don't give in to the fear.
Fear leads to anger. Anger leads to hate. Hate leads to suffering.
AMCs lead to anger, hate, and suffering.
The sky is falling, the sky is falling - anesthesia truly is cyclical. I have seen probably 3 distinct cycles in my 35 years of practice. No reason to think it won't keep happening. Supply goes up, demand and compensation go down. People stay away from the field. Supply goes down, demand and compensation go up.....It's kind of hard to believe the same doom & gloom when the exact same sentiment has been repeated for the last 30 years...
And with talk like "coming of the Ice Age", you make it sound like there is no backup plan. Even if the sky falls for anesthesiology, a CC fellowship is only 1 year. Problem solved.
Great Britain has some AA-type practitioners with very similar scope of practice to US-educated AAs. A couple of our US AA schools have elective rotations over there. CRNA's are nowhere to be found in merry old England.there are crnas in europe. same model as here. I think in great britain they are called oda. Operating department assistant
Are you one of them?maybe
I know employed docs that love their AMC job, however. Normal call, hours, and making $450K W2 per year. Benefits not that great, but a very good job overall.
Most doom and gloomers feel like they lack control and have frustration from that.
Most likely, they are poor businessmen, lack interpersonal skills, generally lack confidence, or are just trolling. Maybe a combo of all 3.
There are ways to compromise with market forces and get what you want without being a Chicken Little.
I suspect that there were Romans that told themselves the same thing when the saw the visigoths climbing the hills of Rome.
Are you one of them?
No AMC is offering 450k w2.. not unless you are taking zero weeks vacation
The sky is falling, the sky is falling - anesthesia truly is cyclical. I have seen probably 3 distinct cycles in my 35 years of practice. No reason to think it won't keep happening. Supply goes up, demand and compensation go down. People stay away from the field. Supply goes down, demand and compensation go up.....

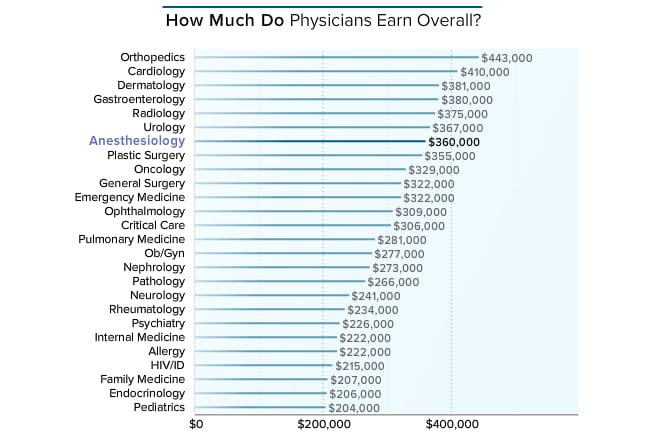
Medscape Anesthesiologist Compensation Report 2016
Carol Peckham | April 1, 2016
Anesthesiologists who responded to this year's Medscape compensation survey disclosed not only their compensation but also how many hours they work per week, how many minutes they spend with each patient, the most rewarding part of their job, changes to their practice resulting from healthcare reform, and more. (Note: Values in charts have been rounded and may not match the sums described in the captions.)
You speak so big. I would love to know how you are immune to all this? I would love to know your practice setting. you are probably the boss' bitch!Most doom and gloomers feel like they lack control and have frustration from that.
Most likely, they are poor businessmen, lack interpersonal skills, generally lack confidence, or are just trolling. Maybe a combo of all 3.
There are ways to compromise with market forces and get what you want without being a Chicken Little.
You speak so big. I would love to know how you are immune to all this? I would love to know your practice setting. you are probably the boss' bitch!
Are you one of them?
No AMC is offering 450k w2.. not unless you are taking zero weeks vacation
Obviously anesthesia has less documentation and less patient contact (at least when they're awake). That's not the point of contention here. The discussion is the tenuous future of anesthesiology and how that will affect your career in the next 20-30 years. Not having patient contact obviously has its upside, but it makes you more readily replaceable, especially when you've been training your replacement for decades. Ownership of patients may not provide complete protection from encroachment, but it's enough for now... whether or not that is worth patient contact is up to you.
New Residency Program Combines Anesthesiology and Emergency Medicine
Residents interested in emergency medicine and anesthesiology can now have the best of both worlds—at the same time.
The American Board of Anesthesiology (ABA) and the American Board of Emergency Medicine (ABEM) launched a combined training option that will offer residents the opportunity to get certified for both specialties.
“The combined training programs in emergency medicine and anesthesiology will reduce redundancies and increase efficiency in the education and training of these residents,” said Barry N. Heller, MD, ABEM President, in a press release. “Furthermore, graduates will be prepared to serve as leaders in either specialty with access to a broader array of career opportunities.”
ADVERTISEMENT
The new program consists of at least five years of residency training. This will be increased to 72 months if a program includes a four-year emergency medicine residency. An applicant may take initial certifying exams for either board after successfully completing the combined education, which is verified by both the ABA and ABEM.
The ABA and ABEM are currently accepting applications for this combined training. Residency programs looking to offer this option must first be approved by both the ABA and ABEM before recruiting residents.
“This ABEM and ABA collaboration provides opportunities for training programs to enhance the depth and breadth of multidisciplinary residency training, which can enhance patient care in systems-based medical practice,” said James P. Rathmell, MD, ABA secretary, in a press release. “It also addresses a demand from residents interested in both emergency medicine and anesthesiology.”
yesIf the crna killed the patient without even calling the doc. The doc is automatically responsible?
New Residency Program Combines Anesthesiology and Emergency Medicine
Residents interested in emergency medicine and anesthesiology can now have the best of both worlds—at the same time.
The American Board of Anesthesiology (ABA) and the American Board of Emergency Medicine (ABEM) launched a combined training option that will offer residents the opportunity to get certified for both specialties.
“The combined training programs in emergency medicine and anesthesiology will reduce redundancies and increase efficiency in the education and training of these residents,” said Barry N. Heller, MD, ABEM President, in a press release. “Furthermore, graduates will be prepared to serve as leaders in either specialty with access to a broader array of career opportunities.”
ADVERTISEMENT
The new program consists of at least five years of residency training. This will be increased to 72 months if a program includes a four-year emergency medicine residency. An applicant may take initial certifying exams for either board after successfully completing the combined education, which is verified by both the ABA and ABEM.
The ABA and ABEM are currently accepting applications for this combined training. Residency programs looking to offer this option must first be approved by both the ABA and ABEM before recruiting residents.
“This ABEM and ABA collaboration provides opportunities for training programs to enhance the depth and breadth of multidisciplinary residency training, which can enhance patient care in systems-based medical practice,” said James P. Rathmell, MD, ABA secretary, in a press release. “It also addresses a demand from residents interested in both emergency medicine and anesthesiology.”
He won't be needing your help for closed reductions. Neither will he be sending patients up to surgery with a 22 gauge IV. He will know how to rapidly transfuse blood and fluids using a level one. So you won't be getting a hypovolemic and hypotensive trauma patient to the OR.What in the hell? How do these 2 specialties overlap at all other than being hospital based? This is crazy. I guess the newly minted ER anesthesiologist won't be calling me anymore for middle of the night difficult intubations.
Right on the money.That's not speaking big at all. I'm no alpha. I don't get my rocks off my telling surgeons to take a hike, putting nurses in their place, or flipping the bird to hospitals.
Just do my best and try to be kind and do a good job.
Good work finds good people. I sincerely believe that, and I see it every day.
As far as my practice setting, you're always free to PM me.
He won't be needing your help for closed reductions. Neither will he be sending patients up to surgery with a 22 gauge IV. He will know how to rapidly transfuse blood and fluids using a level one. So you won't be getting a hypovolemic and hypotensive trauma patient to the OR.
That's not speaking big at all. I'm no alpha. I don't get my rocks off my telling surgeons to take a hike, putting nurses in their place, or flipping the bird to hospitals.
Just do my best and try to be kind and do a good job.
Good work finds good people. I sincerely believe that, and I see it every day.
As far as my practice setting, you're always free to PM me.
Unfortunately if I went in for surgery at a hospital where they have an ACT model, I will not get a doctor. It will be a Crna and there's no two ways about it. Yes the Crna will be supervised etc. but what if I just wanted a doctor solo? Unless these groups go to an all MD model. But then the docs would have to take a pay cut. There lies the problem and our lack of interest in fighting the proliferation of the Crna profession. We need them. Then we teach them. Then they turn around and say I'm so good I don't need you any more.
Can someone explain why we teach them to do everything including intubations, extubations, blocks, etc.? They are not residents. I don't see why they need to know how to independently administer an anesthetic when they are ostensibly there to keep things at cruising altitude while the attending steps out of the room.
Many, if not most, academic institutions have very collegial relationships between MD and CRNA. The academic culture embraces all those apart of it. Regarding why MDs teach sRNAs, I actually inquired about this on the interview trail.. which probably got me blacklisted from certain programs. I couldn't wrap my head around why the attendings taught the srna/crnas.
"It's just the way it's always been. We need them to do things the right way. They are a part of our future."
That is correct. Unfortunately, some surgeons are bullies, and do not respond to kindness.Right on the money.
Very few relationships, at work or otherwise, need to be adversarial. If they are, it's probably you.
You are only scratching the surface here. Most employed attendings would never tell you anything negative about CRNAs, unless they want to put their jobs at risk. Same goes with the way they behave with "their CRNA colleagues". It's Omertà. You guys are not insiders. Same goes for the CRNAs or midlevels in general; many more are militant than actually show it in the daily interactions.Many, if not most, academic institutions have very collegial relationships between MD and CRNA. The academic culture embraces all those apart of it. Regarding why MDs teach sRNAs, I actually inquired about this on the interview trail.. which probably got me blacklisted from certain programs. I couldn't wrap my head around why the attendings taught the srna/crnas.
"It's just the way it's always been. We need them to do things the right way. They are a part of our future."
That is true. Some will not respond to kindness. But you must not respond with anger. Anger leads to suffering... and it is not he who suffers... it is you.That is correct. Unfortunately, some surgeons are bullies, and do not respond to kindness.
Outpatient specialists don't routinely have to answer to HMOs or other insurance entities, unless you are self employed. If you're self employed, then you run your own business and that's its own pros/cons discussion. I would argue that if you are able to stomach the inherent "risk," and are willing to take on the additional work, then starting your own practice in a favorable local market is the way to go. It's not just about encroachment - it's about flexibility and patient perception of value, which then inherently translates into tangible value. Again... whether that is worth the patient contact is up to you.Therein lies the crux of the argument among young med studs on whether to choose Anesthesia/Rads/Path/EM vs other fields. Would you rather relinquish ownership of a pt, not succumb to decades of doom and gloom of being replaceable, and have a "relatively easier" practice management lifestyle OR choose to own patients, answer to them and their HMOs, MCOs 24/7, and bask in the "safety" from midlevel encroachment. Though you can argue what the difference is between CRNA vs NP/PA etc...
They also know what's down, depending on the year...some of you guys and your crystal balls.. Talking this and that about other specialities. I know FM docs who switched into anesthesia. And vice versa. The nephrologist I worked with absolutely kills it $$. Yes he works hard. The pediatrician I rotated with also kills it. He works hard too. Anecdotal? Sure. But the money is out there if you want it. Nobody is going to hand you millions. Work is Work. It probably will suck. Hopefully you'll enjoy some of it. You can't finish training and immediately land your dream gig in your dream city with the perfect setup. Know what you're getting into and set realistic expectations. I'm glad I'm not crunching numbers and filing taxes during busy season like some of my miserable accountant friends. Now my real estate friends.. they know what's up..
I agree. Professionalism is key, otherwise, between a surgeon and an anesthesiologist, the former will almost always win with the bean counters.
Wow, so many militant CRNAs in the comments section of that article!An interesting article on our state of affair:
http://www.houstonpress.com/news/go...t-leaves-the-room-during-an-operation-7842230
Take home points:
-If you're medically directing and the CRNA f's up while you're not in the room... and even if you come to the rescue and do everything right, you can be held liable for the bad outcome.
-If you hire CRNA's and they do something wrong without consulting you (even if you didn't sign the chart), you can be held liable for not controllibg your CRNA's well enough.
-Stay vigilant my friends. You may be directing 4 rooms, but you must have a pulse on each room at all times.
