The vaccine just gives you covid19 spike proteins. Harmless protein. It doesn't do jack sh1t to your long term health. It's not "probably", it definitely has a lower risk than getting replicating active viruses wreaking havoc in your body.
Damn, people are a bunch of irrational wimps.
The vaccine is definitely not no-risk, but it is as low a risk given the current circumstances and we know nothing that should stop the current vaccinations. The serious side effects are still within the rare (1:200,000) if not the very rare (1:2M).
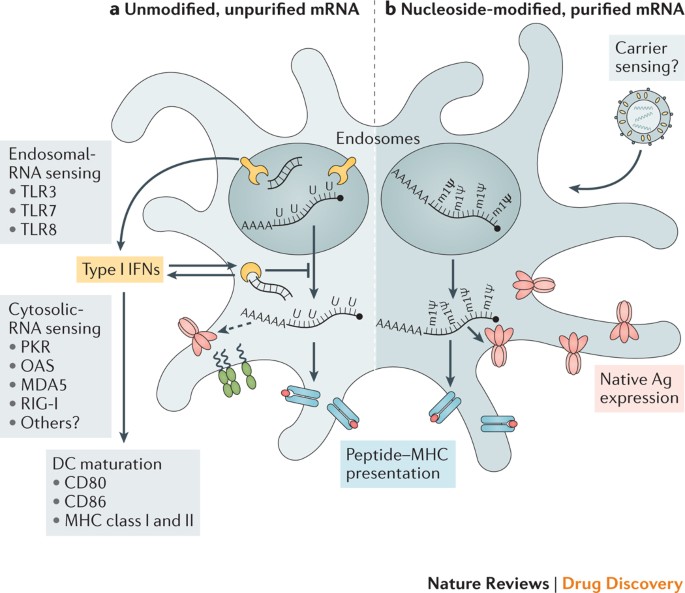
mRNA Vaccines 101 (Written before COVID and actually was addressing Zika):
mRNA vaccines represent a promising alternative to conventional vaccine approaches, but their application has been hampered by instability and delivery issues. Here, Pardi and colleagues discuss recent advances in mRNA vaccine technology, assess mRNA vaccines currently in development for cancer...

www.nature.com
It's hard to argue that this is not objective in presentation (maybe even a bit too positive).
There are downsides as the article writes: those with autoimmune responses have a plausible chance of reacting catastrophically to an mRNA vaccine. And in longer term situations, mRNA naked has a probability of causing autoimmune reactions if found in the improper cells. This work was early 00s, and I remember the seminars on those issues as finding therapeutic spinoffs from the Human Genome Project was the rage at the time.
Yes, the vaccine *potentially* can do quite a bit in long-term health and we all hope that this remains theoretical, but we've not had enough time to really test this vaccine over a time period to weed these problems out. The guy at NIH who is usually the most tech progressive on these matters, Dr. Michael Kurilla, either abstained or voted against the current wording on grounds that the age categories really make a difference on risk vs. benefit given what we don't know about the long-term use. That wasn't lost of any of us. But this is all theoretical at present except for the anaphylactic which impacts Pfizer.
Also, on VCIP, this is a reminder that the program was instantiated due to widespread observations of TDwP associations with encephalopathy and other neurological issues which is why we have TDaP and Td today. The last two EUA's, Dengvaxia and AVA, were extremely problematic and the only reason that they are not included in the VCIP statistics is that uniformed do not report through that system and Dengvaxia was observed elsewhere as we do not have endemic dengue. I personally had the AVA 6 injection hell as that was expected of my generation working in a lab without any serious effects (and arm and abdominal pain around the injection is annoying but not serious).
I am definitely not anti-vaccine, but I definitely would be a bit less of an overt cheerleader until we get enough vaccinated and a long enough observation period to really get these to normal approval. But in the interim, it is a nuanced presentation, and we do owe it to our patients to be given a fair choice. For me, it's absolutely necessary for front-line clinical workers, institutionalized residents (nursing home, prison, group home), miners, bartenders, and those who interact with the stupid parts of the public like the police. A great case can be made for geriatrics in general. Pediatrics is much less of a good argument unless they have underlying conditions. I think it's not a clear-cut case for adults who are normally healthy without underlying conditions.